|
|
Phase I |
Suhadolnik, et al. and others, Temple U |
|
Komaroff et al., Harvard U |
|
|
Klimas et al., U Miami |
|
|
Phase II |
McGregor et al., Newcastle U. New South Wales, Australia |
|
Pimental et al., UCLA |
|
|
Phase III |
Demitrack et al., National Institutes of Health |
|
Moorkens et al., Antwerp U, Belgium |
|
|
Urnowitz et al., UC Berkeley |
These are some of the key articles that support at least the ideas of Phases I, II, and III. They certainly describe the problems of these phases; they just don't call them phases. It's just a clinician like me who has followed it for ten years who suggests that these may be phases, because of what I see. But in fact, there's quite a bit of literature to support all three.
Phase I. Suhadolnik has published many articles over the past 10 years on the disturbance of RNase-L, which is a defense against viruses and intracellular bacteria and is significantly disturbed and upregulated [more active than normal] in CFIDS. This suggests that this disease is initiated by some intracellular pathogen [disease-causing micro-organism]. It might be a virus, or something like Mycoplasma incognitus and Chlamydia pneumoniae, which are bacteria that live inside the cell, and therefore the body has to defend against them in the same way it defends against a virus. The principal way it defends against them is through this RNase-L pathway.
This RNase-L pathway may be the critical element in initiating CFIDS; it's not sufficient to trigger it, but it certainly seems to be necessary. But anyone with elevated RNase-L is definitely going to have an achy flu-like feeling.
Komaroff was the first to recognize a disturbance of immune function, specifically TH1 suppression, and in this case, suppression of the natural killer (NK) cell, which is part of the TH1 system, suggesting that there is a disorder of T-cell functioning. In his particular set of publications, he was looking more at the TH1 suppression side. On the other hand, Nancy Klimas, an immunologist at the University of Miami, has published a series of articles suggesting that there's also significant T-cell activation, presumably TH2 activation, since TH1 is suppressed. So the pattern emerging in Phase I is significant activation of this RNase-L antiviral pathway, upregulation of the TH2 system, and downregulation of the TH1 system. [The TH1-TH2 system is discussed in detail later in the summary.] That's the immunologic pattern, which suggests some kind of immune system activation against a microbial agent, but also suggests something that's peculiarly disregulating it, that we don't quite understand. And if your immune system is responding to a microbe and is disregulated, it might not be able to handle the microbe properly, in which case, you don't recover from the disease in the normal way. It simply goes on and on and on and exposes you to the next set of problems, and that of course is Phase II.
McGregor and Dunstan of Newcastle University in New South Wales, Australia, were the first to identify a metabolite in the urine of CFIDS patients, coming from bacteria in the gut, that correlated with triad symptoms. [A metabolite is a substance produced when the body metabolizes another substance.] It correlated with brain complaints, with fatigue, and with pain. The first proposed marker for this illness, which they labelled initially CFSUM1, for CFS urinary marker 1, actually correlated with these triad symptoms. Supporting that theory is a wonderful experiment by Pimental and others at UCLA where they took antibiotics and eradicated bacterial overgrowth in the gastrointestinal (GI) tracts of a group of fibromyalgia/CFIDS patients. First they had them fill out 11 questionnaires that measured their degree of brain dysfunction, pain, and fatigue. In addition, they measured breath hydrogen gas, since human beings don't produce hydrogen; it comes only from bacteria in your gut. They found elevated hydrogen gas in 92% of these patients, suggesting that small bowel bacterial overgrowth [unhealthy levels of bacteria] was present in 92%. Then the patients were given broad-spectrum antibiotics long enough to eliminate the overgrowth. And they found, to their surprise, that when they used the questionnaires again to measure clinical condition, these patients had significant improvements in their brain complaints, in their fatigue, and in their pain, simply from eradicating bacterial overgrowth.
Again to emphasize the finding of McGregor et al., there seems to be an ability of xenobiotic metabolites [not produced by the body itself, but by bacteria in the gut], to affect the triad symptoms of this illness. This may explain some of the positive responses to antibiotics reported by CFIDS patients. Though it is usually attributed to action against Mycoplasma or Chlamydia, the benefit may in fact simply come from microbial gut ecology improvement. Or maybe several things are going on.
The Phase III element publications are by Demitrack, Moorkens, and Urnowitz. Demitrack is a psychiatrist at the NIH who, along with his wife, first demonstrated a disorder of the hypothalamus in the deep subcortex, showing that the hypothalamic-pituitary-adrenal axis was downregulated [less active than normal] due to a lesion [area of damaged tissue] at or above the level of the hypothalamus. Moorkens recently published an article showing that growth hormone is similarly deranged [not functioning normally] at the level of the hypothalamus. Urnowitz was the first to show DNA gene rearrangements and DNA expression changes. We think the injury to the areas of the brain that control dynamic hormone response, namely the hypothalamus, and also DNA gene rearrangements, could account for the Phase III elements that we see, because nothing would limit your activities more effectively than knocking out dynamic hormone response. [Dynamic hormone response is the body's capacity to produce greater amounts of hormones when they are needed to meet conditions that increase stress on the body.]
Let's discuss your dynamic hormones. There are four major dynamic hormones. The most dynamic hormone in your body is growth hormone. It's important in controlling basic protein synthesis, and in augmenting protein synthesis under certain conditions, such as exercise, hypoglycemia [low blood sugar], and Phase IV sleep. We think increased growth hormone production during deep sleep is a designed upregulation increase] of liver protein synthesis so you get maximum detoxification at 3:00 a.m. [Liver enzymes, which are proteins, are necessary to neutralize toxins and remove them from the body.] The liver has the highest protein synthesis rate in the body, and you have to get the protein synthesis augmentation around midnight to get maximum detoxification, at 3:00 [if you live on a normal schedule]. If you do not have dynamic growth hormone response, then the following terrible things happen: You lose your protein synthesis; what that means in a big way is that you can no longer heal, and you can no longer get well, you cannot exercise, and you cannot detoxify. And you cannot handle hypoglycemia. [Your blood sugar can fall to levels that make it both physical and mental functioning very difficult, and your body does not respond by increasing blood sugar to normal levels.]
Another important dynamic hormone is cortisol. It's typically higher in the morning, lower in the evening, and it responds also to significant stresses, physical, psychological, or cognitive. If you don't have a dynamic cortisol response, you cannot work; you cannot engage in the workplace; you cannot deal with complexity; you cannot deal with irritating people; you cannot deal with any stress whatsoever. You also cannot stabilize protein tertiary structure under metabolic stresses, because cortisol is important in encoding for heat-shock proteins that stabilize tertiary structures of proteins under metabolic stress. [Proteins are synthesized in the form of long chains. In order to do what they are needed to do, they must first fold themselves into exactly the right shape; this is protein tertiary (third-stage) structure. If there is insufficient cortisol to maintain this tertiary structure, although the necessary proteins are present in the body, they are useless.] And cortisol probably has the biggest effect on the capacity to work.
Other dynamic hormones are female sex hormones, and if dynamic female sex hormone responses are disregulated, then everything that you can think of that can go wrong with female estrus cycles will go wrong, all the way from bleeding too much to not bleeding at all (amenorrhea), to ovarian cyst formation, endometriosis, infertility, and PMS.
And the fourth one is anti-diuretic hormone, which maintains fluid balance in the body [by controlling how much water is excreted in the urine], and if you lose that response, then you pee your brains out, and your blood volume is decreased. Lots of interesting studies have been published to suggest that blood volume is depleted in some CFIDS patients. That probably is the cause of tilt-table positivity in this illness. [The tilt-table test measures orthostatic intolerance or neurally-mediated hypotension, which can cause weakness or fainting when standing, even for short periods, and are associated with reduced blood volume.] It certainly is the cause of low blood volumes as measured by chromium-51 labelled blood studies.
So you lose all of this when you lose hypothalamic function, and you essentially become constrained inside some boundary, and if you try to cross that boundary, you get creamed. We call that the push-crash phenomenon.
Urnowitz's article, initially published on Gulf War Syndrome, but extended to CFIDS later, is really interesting. What he's discovered may be the method by which we change our DNA into better DNA to meet the challenges of a physiologic threat. Under serious stress like a great climatic change or a severe catastrophic epidemic, or simply an indivualized stress, human beings and other primates actually have regions in their DNA that undergo gene rearrangements around particular foci [specific points] within the DNA. These gene rearrangements are like shuffling a deck of cards, looking for a better set of genes to allow the organism to withstand the threat. In other words, this is the genetic basis of human evolution under physiologic threat. It has allowed humans adapt and live in widely different climates. And should there be some cataclysmic event like a meteor hit on the planet, we'd probably adapt and some of us would live on, and this is the mechanism that allows it. This gene rearrangement occurs in some CFIDS patients. It may be helpful in some patients, and in some patients may be somewhat hurtful. The rearrangements are random, so it's sort of like a casino game in which you have to play the cards you're dealt, and some people by chance alone get a really good hand, and some people by chance alone don't get such a good hand. The bad hands are characterized by the ability to code for toxic material. [The new gene arrangement can cause the body to produce toxins that would not otherwise be present.] That may be important in understanding why people can remain ill with this for a long time. They've actually undergone a type of gene mutation.
Urnowitz has also gone on to show that even normal genes are expressed much differently in this illness than they are normally, suggesting that even in the case of normal genes, there's a tremendous change in gene expression that goes on. [A particular gene may have different effects under different circumstances, and CFIDS causes greater variation in gene expression.] Here's another area where antibiotics might actually, interestingly, help in this illness. Antibiotics like erythromycin and doxycycline actually modulate [alter] gene expressions because they affect protein transcription translation events [the process by which genes direct the production of specific proteins] and therefore would affect gene expression.
These are in my view the key scientific articles that suggest that there's a very interesting set of pathophysiologies going on in this disease, and there does seem to be a sequence, so there's a dominant phase, followed by a different dominant phase, and then followed by a late dominant phase.
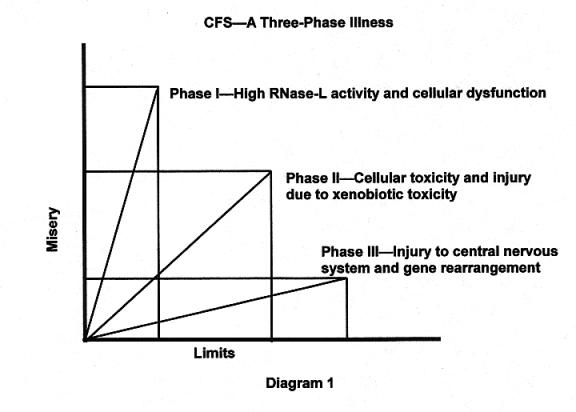
I try to plot this three-phase illness. Phase I is mostly misery and some limitations. This is the phase of high RNase-L activity and cellular dysfunction based upon high RNase-L. You need to know what RNase-L actually does. It's a human enzyme present in every single cell of your body, and when it's activated, it chews up messenger RNA and prevents protein synthesis. It's designed to destroy viral protein synthesis [and prevent reproduction of viruses], but it doesn't know the difference between viral messenger RNA and human messenger RNA. So when it's upregulated strongly enough, it actually destroys human messenger RNA, preventing synthesis of essential human proteins and putting cells into significant dysfunction. They simply can't make the protein enzymes they need to work. The point is that high RNase-L will literally put you on your back.
What's interesting about this enzyme system is that this is a normal enzyme system. It's not a pathological system. It's actually designed to impede viral replication, and you need it when you have viruses trying to replicate [reproduce]. But of course preventing protein synthesis makes you feel bad, and so while RNase-L is holding down viral replication, you don't feel very good. So in order to understand why CFIDS patients can do so poorly and yet kind of look okay, you need only look at the fact that some of the things that are going wrong with them are things that everybody has go wrong some of the time [when their bodies are fighting viruses], It's just that in CFIDS patients, this process is more sustained and perhaps even disregulated, and they have some other things thrown in. They have a disturbed physiological function rather than a true destructive pathology, which is why they look different from MS patients or cancer patients.
I never will forget, in 1991 I was sitting in a hotel room with Dr. Suhadolnik when he was first presenting these data on RNase-L. He was showing these electrophoretic gels. [Electrophoresis is a method of separating out different chemicals in a mixture; they appear in different places on a gel slide.] You incubate human lymphocyte cytoplasms with a target messenger RNA. [Lymphocytes are immune system cells, and cytoplasm is the substance of the cell, excluding the nucleus and the cell wall. The purpose of the experiment is to see what RNase-L does to the target RNA.] The RNase-L digests the target RNA into little pieces, and the pieces migrate all the way down the gel, and you can basically see little pieces of the RNA target displayed on the gel. He showed the gels of CFIDS patients, and of course he's a wonderful man and a wonderful scientist, and he's all excited about these blank gels he's showing to the group huddled in the hotel room. He says, "Look! Look, do you see this? Do you see this?" And I looked at these gels, and I said, "But Robert, there's nothing on the gel." And he said, "I know, I know; don't you understand?" I said, "No." He said "Well, it's because the RNase-L digested everything, digested it all completely, into such little tiny pieces that they had migrated completely off the gel into the gutter." He went on to say that the RNase-L of these patients will digest in 60 seconds a target ribosome that the RNase-L of a normal human being cannot digest in 60 minutes of incubation. [Ribosomes are spherical bodies within cells that are the sites of protein synthesis.]
When I finally understood that this tremendous rate of destruction of messenger RNA was going on, it suddenly dawned on me; I went from not understanding why these people were so sick to understanding why they were so very sick. And I remember the hairs standing up on the back of my neck as I realized, "I now understand this. I understand why they can be that sick, yet not really look like they should be that sick, because they have a disturbed physiologic system that's simply over-producing RNase-L and destroying messenger RNA" [and their cells are so badly damaged that they can't function].
Phase II--you'll notice that it's still pretty miserable, but there is also increasing dysfunction. This is the triad phase, and it's characterized by xenobiotic toxicity [from toxins foreign to the body]. This involves the gut toxins described by McGregor and the UCLA group. The organ with the greatest rate of protein synthesis, which would be most affected by RNase-L is the liver, and if RNase-L is chewing up messenger RNA and destroying the liver enzymes that are used to detoxify, how would you detoxify the portal circulation? [The portal circulation takes blood from the small intestine to the liver. This blood carries nutrients absorbed from the intestine, and also toxins from the intestine. A healthy liver detoxifies this blood before it circulates to the rest of the body.] And the answer is, you wouldn't. What would the portal circulation do to you if you didn't detoxify it? It would make you really sick. But sick in a different way; it would make you poison sick; you'd feel as if you were poisoned rather than sick with a virus. That is exactly what happens, and that is what we think really characterizes this transition from a viral phase to more of a poisoning phase.
And then the last shift is to Phase III where there's a big drop in misery, because miracles do happen, and the miracle is that RNase-L seems to downregulate. That improves xenobiotic toxicity problems, and then you're left simply with the damage done [by these toxins] to the brain, the hypothalamic area, the controller of these dynamic hormones. You also have these DNA gene rearrangements. So you're still left without the processes that allow you to exceed boundaries. So you have a big boundary problem, but you don't feel so miserable.
The Recovery Trajectory
The recovery phase. Patients sometimes ask, "Do you ever really get over this?" And I think you actually do. And they ask the question, "Who gets over it the best?" And the opposite of that: "Who is least likely to recover?" Once they make it to Phase III, the people who are continuing to get better and better are the people who are probably going to get out of this, or at least largely out of this, and they're in yellow [in the diagram]. And then those whose functions are declining over time, they're the ones that probably aren't going to get out of this. They're either stable--in the middle--or they're just getting worse and worse from a functional standpoint. And the question is, what people are usually yellow [improving], and what people are usually green [not improving]? And the answer is, teenagers are usually improving. As I look back over my charts and ask the question of how teenagers fare with this disease, I'll tell you, they get as sick as adults. They can be homebound for five years. They can be really sick, and I've even seen them die. But when I ask the question, "Well, how many never really made it out of this disease?" I can only think of two out of maybe 20. So it seems that 90% of teenagers, once they get to Phase III, seem to recover.
However, if you go to 40 and older, the numbers are almost the opposite of that. Only 10% truly recover, unless they get well within the first couple of years. If they stay ill for very long--meaning maybe five years or longer--then it's rare to see them recover. They can be stable; they can get through the first two phases pretty well, but they still have a functional impairment. People between 20 and 40 are kind of a mixed group. They're better than the people over 40, but they're not as good as the kids under 20, and they tend to resemble the adults over 40 a little more than the kids under 20.
I've puzzled over this for years, wondering why the kids do so well, and the adults do so poorly. I think the difference may be growth hormone. I'll tell you a story that always challenged my thinking on this. When I was a sophomore in medical school, my first rotation was in pediatrics, and the first patient I took care of was a young girl who had been hit over the head with a crowbar by her father and suffered a severe cerebral contusion [bruising of the brain] and had significant brain swelling, and it looked as if she was going to die. They took her to emergency neurosurgery, and I assisted the neurosurgeon in taking part of her skull off and sucking half of her frontal lobe out of her brain, simply taking a suction device and sucking it out. And at the end of the procedure, I was aghast, and I turned to the neurosurgeon, and I said, "How can you do this? Wouldn't you just leave her as a vegetable?" The reason for doing that, by the way, was to create a space for the brain to swell into so the pressure [on the brain stem] would not be great enough to kill her. And he simply said, "She's ten years old. If she were 25, she would be a vegetable; it would be like a lobotomy. But at ten years old, they do fine, if they survive the acute injury." I always remembered that, and if you've ever done any reading on the issue of stem cell research or growth factor research or growth hormone research, one gets the feeling that this is the direction of medical research into how we will resuscitate injured organ systems, whether it be brain or heart or whatever. The controlling factor in this resuscitation capacity, interestingly, may not be stem cells, unless you're over 60, when you may need stem cells. The controlling factor may actually be growth hormone, and a ten-year-old has ten times more growth hormone than even a 30-year-old does.
[Stem cells are undifferentiated cells found in human embryos. After they are differentiated, cells can only develop into one specific type of tissue, but stem cells still have the ability to develop into any kind of tissue. Therefore, they have the potential for healing any part of the body.]
And again since CFIDS affects the growth hormone dynamic, the only CFIDS patients who might have enough growth hormone left to recover completely turn out to be teenagers and children.
The Physical Exam, Immune Activation
Lymphodynia [tender lymph nodes]--80% to 90%
Crimson Crescents--80%
Fever--25% have fevers above 99.4
There's an interesting set of findings on physical examination of these patients, and they've been fairly consistent over the years.
There's evidence of immune activation, and that evidence is in the supraclavicular lymph node area and the posterior cervical chain; that's in the lymph node area at the back of the neck and right above the clavicle [collarbone]. A majority of patients--in the 80% to 90% range--are tender in these regions.
It seems that the degree of lymphodynia has diminished over time, suggesting that for many patients, this illness is changing. Since this tenderness is a Phase I element, I think a lot of my patients have progressed past that stage.
A crimson crescent, which is a band of purple tissue on either side of the uvula [the small, fleshy projection hanging at the back of the roof of the mouth], over the soft palate, is seen in about 80% of patients. Fever is another one that has changed. When I first took this data about ten years ago, fully a third of my patients had a low-grade fever, defined as 99.4 or higher in the morning, but it seems to be declining. Again, this is a Phase I element. I think it's down to about 25%, maybe continuing to fall somewhat. The very fact that Phase I elements are declining suggests that we may have had an epidemic of CFIDS, which is one of my hypotheses on this problem going back to Tahoe days, when we had a true epidemic of about 265 people. But other people have looked at epidemiological curves to suggest that the epidemic of CFIDS began in the late 70s, peaked in 1987, and has been in a slow decline ever since. These Phase I indicators also seem to suggest that, since they also seem to be declining.
The Physical Exam, Subcortical Brain Injury
Vestibular Dysfunction [balance problems]--94%
Hyper-reflexia [abnormally strong reflex responses]--80%
Subcortical brain injury. Vestibular function is by far the most sensitive indicator. ["Vestibular" normally refers to the vestibular structures in the inner ear, which are important in maintaining balance. Dr. Cheney uses the term "vestibular disorder" for these balance disorders, even though they are caused by the brain rather than the vestibular structures.] We see the dysfunction on three simple tests. One is called the Rhomberg; one is called the tandem stance, and the third is called the augmented tandem stance. If you're under 50, you should be rock-steady on each of these three tests. If you're over 50, you might be a little unsteady on the third one. But you should be okay on the first and second ones, even up to the age of 75. Komaroff has published a paper on platform posturography results, which is a very sophisticated test of vestibular function developed for NASA, that demonstrates that the reason for vestibular dysfunction in CFIDS is deep brain injury, that is, subcortical injury.
Then there's hyper-reflexia, seen in 80% of patients. It tends to begin in the ankles and knees and then moves toward the head. It's very common. You can even see unsustained clonus (a double vibration upon tapping), particularly at the knees or ankles. Subcortical injury can typically produce hyper-reflexia. Hyper-reflexia is a feature of multiple sclerosis for exactly the same reason. You see hyper-reflexia in 20% of normal people but 80% of CFIDS patients, so it's not an abnormality of itself, but rather a more frequently occurring abnormality. The exception is when you see this unsustained clonus, and that is never normal. We see that in about 5% of patients.
The Physical Exam, Metabolic Disturbances
Shortened breath-holding--70%
Poor oxygen transport--92%
Fingerprint destruction--50%
Sub-normal temperature30% have temperatures below 98.6
Low systolic blood pressure--50% have systolic BP below 100
Orthostatic BP or pulse changes [changes on standing up]40%
Hypertension is very rare--less than 2%
There are lots of metabolic disturbances, and we'll go in detail over some of these, but one interesting one is shortened breath-holding. If you ask CFIDS patients to hold their breath after emptying the lungs--relatively emptying the lungs and holding their breath as long as they can--they don't hold their breath nearly as long as normal individuals. More interesting than that is that if you put a pulsoximeter on their finger and have them hold their breath, they do not desaturate in 70% of cases. [Blood oxygen levels are not reduced.] When you have someone expire all the air out of their lungs and then hold their breath as long as they can, the only way they can get oxygen [into the tissues] is to pull it off the hemoglobin molecule [which bonds to oxygen in the lungs and transports it to the tissues], and therefore desaturate the hemoglobin molecule. Seventy percent do not desaturate, which is pretty amazing. What that means is they have plenty of oxygen in their blood, but it will not transfer into the tissues under conditions when the tissues need oxygen.
What would happen if you could not transfer oxygen into the tissues? For one thing, you would have fatigue, and that is not the only thing. Pain comes to mind, and another thing that comes to mind is micro-organisms that are facultative anaerobes, that is, organisms that like reduced oxygen-saturation conditions. [Facultative anaerobes are organisms that grow best in the presence of free oxygen but are capable of growth in the absence of oxygen.] Yeast is a facultative anaerobe; it doesn't like oxygen. Mycoplasma bacteria are facultative anaerobes. Chlamydia pneumoniae is a facultative anaerobe. Yet here we have a situation where patients are not transferring oxygen, so it sets up ideal conditions for these sorts of organisms, which is intriguing, since these organisms are very commonly seen in CFIDS. The question is why. One good possibility is that there is insufficient oxygen transfer into the tissues.
Fingerprint destruction. I think we were the first to see that CFIDS patients often don't have any fingerprints. About 10% literally cannot be fingerprinted at all on any of their digits. Up to 50% of them are somewhat affected, and 50% have normal fingerprints. If you biopsy the tissue [make a microscopic examination of surgically removed tissue], they show various pathologies in the dermis [skin] that I think explain some of this. They show lymphocytic perivasculitis [inflammation of blood vessels], which is a type of immune activation phenomenon that could produce problems of nutrient supply to the dermis. They also show punched-out lesions in the fibroblasts [cells that produce connective tissue], suggesting that they may not be making collagen correctly. That could definitely affect fingerprints. So collagen synthesis could be affected. Fingerprint destruction is quite interesting and quite unusual and is seen even in 20-year-olds with CFIDS. I asked a deputy sheriff how often it was they could not get fingerprints from some-one, and his answer was, "Almost never."
Subnormal temperatures. About 30% have low body temperatures. The percentage with fever seems to be going down, but the percentage with subnormal temperatures seems to be going up, which is, I think, consistent with the transitioning to Phase III.
Low systolic blood pressure [the higher number]; 50% are below 100. Orthostatic blood pressure or pulse changes in about 40% [Standing up causes changes]. All of this is consistent with low blood volumes, common to this illness, and with adrenal insufficiency. Hypertension [high blood pressure] is extraordinarily rare, less than 2%. I do see it, and when I see it, it's almost always familial; the patient's first-order relatives also have high blood pressure, and the CFIDS patient's hypertension is usually not very severe.
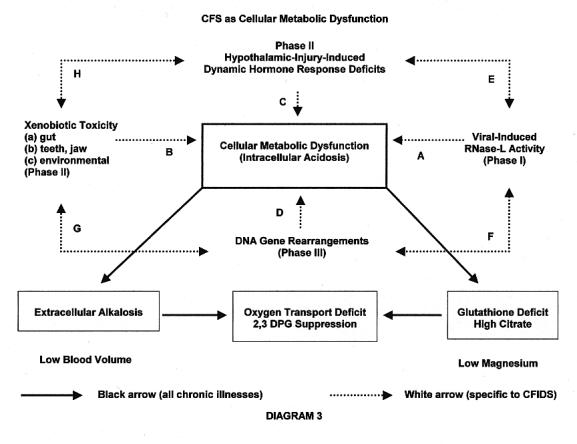
This is a diagram, a sort of recapitulation of what we've been talking about. It's a diagram that gets progressively more complicated. The center of gravity of this disease is a disturbance of cell function that is best described as a mitochondrial dysfunction or energy production dysfunction, with an associated intracellular acidosis. If the mitochondria are not working very well, the cell will become progressively acidic. By the way, this particular cell dysfunction is not unique to CFIDS. You could see this kind of cell dysfunction in almost any chronic medical condition. You could see it in rheumatoid arthritis, AIDS, cancer, lupus. Any chronic medical condition of significant effect is going to degrade cell function and potentially disturb energy production at the cell level. That is why chronically ill people look strangely alike.
What we're talking about here is how CFIDS causes this dysfunction. So this white arrow [point A] is CFIDS-specific, but this blue area [other parts of the diagram] is not specific to CFIDS. Some-one came up to me during the break and said, "I have rheumatoid arthritis, and I have fatigue." Well, they may have this part [cellular dysfunction], but they may not have some white arrows here that are CFIDS-specific. The first thing in Phase I is virally-induced RNase-L activity. That seems to be the necessary condition to initiate CFIDS. RNase-L will destroy messenger RNA, reducing protein synthesis and beginning to degrade cell function. You feel as if you caught something, and you often have other evidence of some immune activation state, be it sore throat, swollen glands, low-grade fever, etc. I should add that there are a minority of CFIDS patients who do not exhibit this acute onset of a viral syndrome; they have a more insidious development [slower and less easily noticed], and that may simply be an infection that is more subclinical. [The symptoms aren't severe enough to be detected in a physical examination.] But 70% seem to be clinically expressed, and this seems to be the big system involved.
If RNase-L activation continues long enough and high enough, it will degrade liver function, and you get xenobiotic toxicity, primarily from the portal circulation, that is, the gut. The liver has the highest protein-synthesis rate in the body; therefore it's going to be really affected by RNase-L. There is a condition called Reye's Syndrome in children, which is a recapitulation of exactly this phenomenon, in which a child gets a viral infection and just as they're recovering from the viral infection, they lose their liver function. That transition from viral infection to liver dysfunction is exactly this transition [from Point A to Point B]. But I don't want to limit xenobiotic toxicity to the gut alone. There could be other sources of toxins involved, such as toxicity from the teeth, particularly root canal teeth, or jawbone osteo-necrotic lesions [infected bone tissue in the jaw], which can be very toxic. There are also toxic environments. So if you lose detox systems, you lose protection against not only the portal circulation; you potentially lose protection against other sources of toxins. But I would like to emphasize that everybody has a gut, and everybody has a poisonous portal circulation, so under this particular set of circumstances, everybody's got a problem from the gut, but there may be some individuals who have additional problems [from environment or teeth and jaw] added on to it.
The next problem, which is recapitulated in Reye's Syndrome and very much recapitulated here, is that the xenobiotic toxins, which are fat soluble, enter the brain, and the place they enter the most is the hypothalamus, because the hypothalamus has the leakiest blood-brain barrier. The reason for this is that the hypothalamus, unlike other areas of the brain, must monitor hormone levels in the blood in order to control the body's hormone levels. So toxins in the blood breach the blood-brain barrier to the greatest extent in that area. So there's a reason for these toxins to reach the hypothalamus specifically and be concentrated there before other areas. In the areas right around the hypothalamus, you have the limbic structures, the hippocampus, site of short-term memory, processing centers, vestibular apparatus, mood centers. You have the whole array of processing centers that seem to be afflicted in this disease, so there could be an expanding array of injury as these toxins flood the brain.
Injury to the hypothalamus damages your dynamic hormone responses, particularly growth hormone, cortisol, female sex hormones, and anti-diuretic hormone, and all of the problems that follow tend to be extremely limiting on your activity levels.
By the way, each of these arrows, in turn, is affecting cell function. Cell function is affected here [point A] by RNase-L activity destroying messenger RNA and preventing production of necessary enzymes. These xenobiotic toxins actually poison the same enzymes [point B]. The loss of growth hormone [point C], which controls protein synthesis, affects those enzymes. With the loss of cortisol dynamic [point C], you lose the heat-shock proteins that stabilize their tertiary structure, so they become unfolded and don't work as well. So essentially all three arrows [A, B, and C] are progressively affecting enzymatic function within the cell, so they're increasing cell dysfunction.
The final one is the DNA gene re-arrangement that Urnowitz discussed, a sort of shuffling of the deck. If you get a good hand, maybe this even helps you. However, if you get a bad hand, you may actually be coding for your own personalized toxin at the DNA level. [The new gene arrangement may direct the cells to produce new toxins that would not otherwise be present.] So you're getting a personal toxin as opposed to some xenobiotic toxin. The only good news here is that if this toxin is really, really bad, it will typically kill the cell that generated it. So we think this [point D] does not generate the degree of toxicity that this [point B] does. It's a milder form. So it's sort of like, once you reach Phase III, you feel mildly sick rather than horribly sick, which this [point B] is capable of causing.
So those are the four arrows of CFIDS. This is how CFIDS damages cell metabolism, and you can see how one problem can foster the next problem which fosters the next problem. But the first problem [damage from RNase-L] doesn't necessarily go away. It can actually stay there reverberating in time, and you may end up with all four arrows acting at the same time. They also interact with each other. Sometimes things going on up here make this worse [point E]. For example, loss of cortisol dynamic upregulates the immune system, creating an increased set point [base line] for immune reactivity and increasing RNase-L activation. And DNA gene re-arrangements can do any number of things regarding this [points F and G]. Loss of growth hormone, which would impair liver function, would allow xenobiotic toxicity from the gut, the mouth, and the environment to be greater [point H]. So they set up feedback loops that are vicious circles making the various problems worse.
If you look at this, you wonder how you would ever survive this, or how you ever get better. It certainly shows that some-one with CFIDS is going to have a very long and tough illness and a tough road ahead of them.
Now come the black arrows. The black arrows are not CFIDS-related. They're simply related to disturbed cell function and mitochondrial dysfunction and intracellular acidosis. Therefore, they can be seen in other chronic illness as well. The first problem is that with intracellular acidosis, you get a compensatory extracellular alkalosis. The body does that: one part of the body gets more acidic, the blood gets more alkaline to balance it out. Alkaline blood inhibits oxygen transport; as the blood becomes alkaline, it inhibits oxygen transfer rates.
Mitochochondrial dysfunction, reducing ATP generation, is linked to glutathione deficiency by the Gibbs free energy equation. [The energy produced by metabolism of glucose is contained in the chemical bonds of adenosine triphosphate (ATP), which transfers it to where it can be used.] The Gibbs free energy equation says that the energy available to do work in the cell is equivalent to the glutathione concentration. [Glutathione is a peptide composed of three amino acids, cysteine, glutamate, and glycine. Like proteins, peptides are composed of amino acids, but peptides are smaller than proteins. In addition to its role in energy production, glutathione is the most abundant and most important anti-oxidant produced by the body and is a powerful detoxifier.] If there's a reduced energy available to do work, there will always be an equivalent reduction in glutathione. Glutathione reduction induces an increase in citrate levels, which can inhibit 2,3 DPG. Citrate is a very potent inhibitor of 2,3 DPG in the red cells. [Hemoglobin in red blood cells bonds to oxygen in the lungs and transports it to the tissues. 2,3 DPG (2,3 diphosphoglycerate) is a chemical that is necessary to allow the hemoglobin to release the oxygen so it can enter the cells.] That would further reduce oxygen transfer at the hemoglobin level. I call it the double hit to oxygen transfer, coming from two directions [alkaline blood and reduced 2,3 DPG]. It's bad enough that you have this disturbed cell function, but there's something else going on that even denies you oxygen to make energy.
At this point, the body actually begins to fight back a bit. One of the things it does is to reduce the blood volume. In medical textbooks, there's a whole chapter called "Contraction Alkalosis." It says that as the blood becomes alkaline, the blood volume will actually be reduced, and what happens then is that the blood becomes more acidic, because it perfuses tissues less well and therefore gains back some of the acidity. [I think this means that when the blood volume is reduced, it doesn't penetrate the tissues as well, and since it has less contact with acidic cells, it doesn't continue to be so alkaline in an attempt to balance the intracellular acidity.] It's a way of balancing out this terrible acidosis, and that may explain why David Bell [who treated a CFIDS outbreak among children in Lyndonville, N.Y. in the 1980s] made this comment to me once; he said, "When you try to fix blood volume depletion with these patients, it doesn't always help them very much. It's as if they want to be volume-depleted." And the reason their systems attempt to be volume-depleted is that they're alkaline, and they can't transfer oxygen unless they're volume-depleted. It may also explain the failure of the Johns Hopkins group to show long-term benefit from using Florinef to treat volume depletion. [Florinef (fludrocortisone acetate) is a synthetic adrenocortical steroid hormone used to normalize blood pressure.] They failed to show benefit on a double-blind, placebo controlled trial. It should have helped since those patients had volume depletion, but not if the volume depletion is a compensatory mechanism. [A double-blind, placebo-controlled study is one in which neither the researchers nor the patients know which patients are getting the drug and which ones are getting the placebo.]
Citrate; you can raise 2,3 DPG levels by dumping citrate in the urine. We measure citrate in the urine all the time, using chromatographic techniques [a method of separating and identifying chemicals in a mixture], and CFIDS patients' urine is always elevated in citrate. Their bodies dump citrate like crazy to keep it from being elevated in the blood, which would be catastrophic. But citrate binds magnesium; it's a powerful magnesium binder, so excreting citrate causes magnesium depletion. There's been quite a bit of controversy about magnesium deficiency. Some people say CFIDS patients are deficient; some say they aren't, but a recent publication by Greta Moorkens out of Belgium has really solved the mystery. What she has shown is that if you use the gold standard [most reliable] methodology, such as magnesium loading tests, 50% of CFIDS patients are deficient in magnesium. Furthermore, in half of those people, you cannot increase magnesium to normal levels with any amount of magnesium you give them, suggesting that they're leaking magnesium out of the cell faster than you can get it in. Of course, if you're leaking magnesium out of the cell, even the magnesium loading test is a flawed assay [measurement] for determining magnesium depletion. The point is that there is no truly valid test for magnesium deficiency in this disease. It literally arises from magnesium leaking out of the cell. But Dr. Moorkens is the first one who sheds some light on why most of the other tests are flawed. The use of magnesium has always been one of the better treatments for this illness. I think clearly on theoretical grounds, and to some extent on measurement grounds, as shown through Greta Moorkens' work, this is a magnesium-deficiency state which should be aggressively treated, even though many tests for magnesium show as normal, since those tests are invalid.
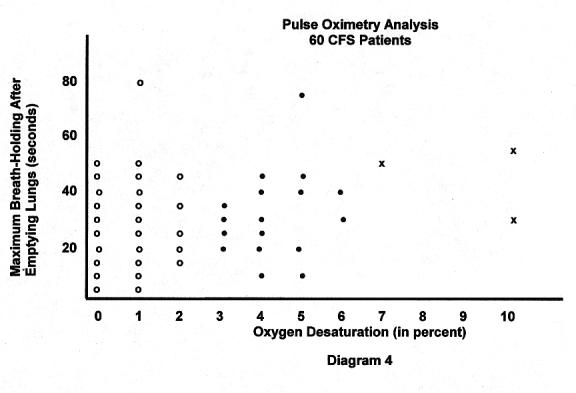
This is the pulse oximetry data. It shows maximum breath-holding, end expiration [after emptying the lungs] in seconds, versus the percent desaturation [reduction in blood oxygen]. Essentially 0, 1%, or 2% is no desaturation, so this [those with 0, 1%, or 2%, shown as "o" on the diagram] represents about seventy percent of this N of 60 [60 research subjects]. Probably these three people here [shown as "x"]are the only normals, and then we have the sort of intermediate group that are showing some intermediate desaturation. But look at this person who held their breath for 80 seconds and essentially didn't desaturate. So they hold their breath; the only way their tissues are going to get oxygen is to pull it off the hemoglobin, and they don't do it. I did a correlation coefficient just to make sure I couldn't explain this based on the length of breath-holding. The correlation coefficient is weak to nonexistent; therefore this effect is not related to the length of holding breath. [A correlation coefficient is a statistical measurement of the strength of a correlation between two variables. In other words, this statistical analysis shows that the lack of desaturation is not explained by the length of breath-holding; therefore it is caused by something else--poor oxygen transport.]
Oxygen Transport
Blood Acid-Base Status (Alkaline blood inhibits oxygen transport)
Red Cell 2,3 DPG Status (Lower 2,3 DPG levels inhibit oxygen transport)
Mitochondrial function
Micro-circulation [blood flow through the smallest blood vessels]
Alkaline blood reduces blood volume
Low magnesium constricts blood vessels
Increased sympathetic tone [the body's stress response, expressed through the sympathetic nervous system] constricts blood vessels
Total blood volume (diminished in CFS)
The things that control oxygen transport are: Blood acid-base status; alkaline blood inhibits transport. Red-cell 2,3 DPG; lower levels inhibit transport. CFIDS patients have both of these problems. Of course, you could have oxygen transfer problems because the mitochondria are not working in the first place. And then there could be micro-circulation problems. Alkaline blood constricts blood volume and could affect micro-circulation. Magnesium deficiency constricts blood vessels, and that can contribute to micro-circulation problems. Increased sympathetic tone constricts; CFIDS patients have been shown to have increased sympathetic tone. And then diminished total blood volume could reduce micro-circulation. So these are the big four reasons to suspect oxygen transfer problems. As we tried to work through some of these four things and doing some other tests, I've concluded that blood alkalosis is the dominant one. Because there are ways to suggest that the other three, although potentially present in individual cases, do not seem to have the breadth of effect that blood alkalosis does. And where does blood alkalosis come from? It comes from diminished cell mitochondrial function and energy production. That makes sense because this is a chronic fatigue syndrome. You don't make enough energy, and one of the consequences of not making enough energy is that blood becomes alkaline, inhibiting oxygen transfer.
Mitochondrial Dysfunction
RNase-L Activity (Inappropriate)--37 kda [the more destructive low molecular weight form]
RNase-L Activity (Appropriate)--Microbial activity (i.e., HHV, Mycoplasma)
Xenobiotic Poisoning--Gut, Root Canal Teeth, Jaw, Environment
Heavy Metals (Especially Mercury)
Growth Hormone Deficiency
DNA Gene Re-arrangement or Alterations in Normal Expression
[Appropriate RNase-L activation would occur when there is an intracellular microbial infection, and the RNase-L is fighting it. Inappropriate activation occurs when the more destructive low molecular weight form of RNase-L is present and also when the infection is no longer there but RNase-L levels remain high.]
Some of the reasons for mitochondrial dysfunction. RNase L activity--inappropriate, such as the 37 kda identified by Suhadolnik. That's certainly going to screw up mitochondrial function, because it's going to chew up messenger RNA necessary for the enzymes that run the mitochondria. You could have appropriate RNase-L activity due to some microbial infection, like HHV or Mycoplasma. These are appropriate reasons to have RNase-L, but RNase-L will still screw up mitochondrial function. Xenobiotic poisoning from gut, root canal teeth, jaw, and environment. Heavy metals, especially mercury. Mercury has a very special binding site, at glutathione peroxidase. [Mercury inhibits anti-oxidant enzymes like glutathione peroxidase.] It can knock that enzyme out. It's a selenium binding site, and mercury hits there. If it hits there, it's going to knock out mitochondrial function. It gets a special warrant [??] there. Growth hormone deficiency, by affecting protein synthesis, is going to affect mitochondrial function. And then of course, DNA gene rearrangements and alterations in normal expression.
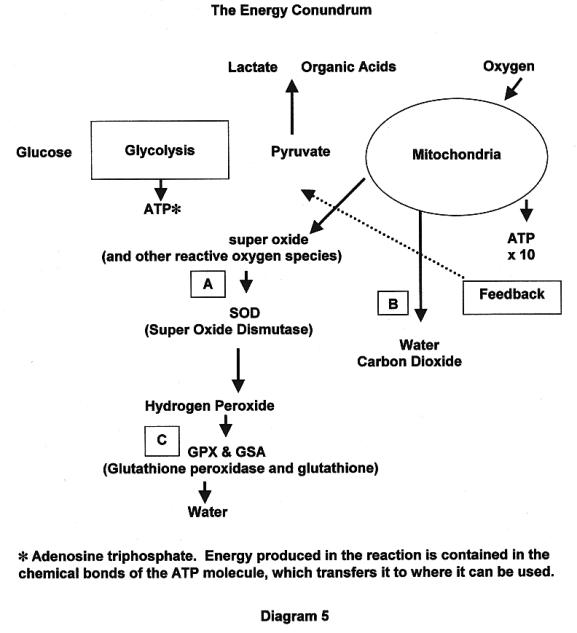
I want to go through the energy production system and show you some of the energy conundrums about it. [A conundrum is a puzzle or a problem.] Glucose is taken into the glycolytic pathway to convert to pyruvate. Glycolysis is the beginning of the metabolism of glucose; the glucose molecule is split into two smaller molecules, each of which is converted to pyruvate. [Glycolysis is anaerobic; it does not require oxygen. It produces some energy, but the aerobic processes that complete the metabolism of glucose produce much more energy than glycolysis.] Pyruvate is taken into the mitochondria and is converted to water and carbon dioxide if it's fully oxidized, releasing vast quantities of energy. You do make a little energy here [ATP (from glycolysis)], but you make ten times more here [ATP x 10 (from complete oxidation)], but to do that you consume quite a bit of oxygen to run the mitochondria. You'll notice that you don't consume oxygen to run glycolysis; we call it, therefore, the anaerobic energy pathway.
As the mitochondria oxidize pyruvate to water and carbon dioxide, it produces some reactive oxygen species [extremely destructive free radicals]. One is called super oxide, which is converted by super oxide dismutase [SOD, a powerful anti-oxidant] to hydrogen peroxide, which is then converted by glutathione peroxidase and glutathione to water. [The pathway on the left (Point A) is a more detailed version of the one on the right (Point B).] The point is that when you make energy, you make these reactive oxygen species. It is very important that they be further metabolized by these enzyme systems [SOD, glutathione peroxidase, and glutathione] down to water. They are so toxic that if your system can't metabolize them further, feedback inhibition will cut off the entire system to save your life. [If too many very toxic substances are produced, the body's protective mechanism shuts down the entire process. Then you only have the energy produced by anaerobic glycolysis, but your body won't produce life-threatening toxins.] The idea is that your body chooses between lower energy and life versus higher energy and toxins and death. This also brings into focus the idea that maybe fatigue isn't as bad as we think it is. Sometimes fatigue could actually be a protective mechanism against damage from these toxins.
This is where mercury hits, right here [Point C]. Lots of CFIDS patients have glutathione deficiency. Even viruses are known to make GPX [glutathione peroxidase] genes that interfere with this metabolic pathway, so viruses have the interesting ability to actually interfere with this system.
I call this the energy conundrum. The energy deficit may actually be a defense mechanism as much as a problem in itself, and the real solution to the energy deficit is to get at the deeper problem.
Note that if the mitochondria can't function, what happens to pyruvate? It is converted to lactate and other organic acids. So one of the indirect measures of mitochondrial function is increasing lactic acid within the cell. That causes intracellular acidosis, from which you get extracellular alkalosis, blocking oxygen transfer. You can directly measure mitochondrial function by measuring the amount of oxygen consumed by that individual; it's a direct measure of mitochondrial function.
There are actually three articles published in the medical literature to support the existence of mitochondrial dysfunction, but what I'm going to show you is data that I personally developed or that I have been working on.
SLIDE--Brain Scan [Not reproduced for this summary]
This is called magnetic resonance spectroscopy [MRS]. It's a marvelous kind of brain scan. It allows us to look at a very small area of the brain called a voxel, which is the three-dimensional equivalent of a pixel a [single dot in a photo]. It's no bigger than eight millimeters by eight millimeters by one millimeter thick, no bigger than the end of this pointer. Although you don't appreciate it, these little arrows are coming out to the side, showing where we're looking at different voxels. There are actually six voxels being examined in this particular brain slice. [A voxel is a cubic millimeter of tissue. MRS can measure the levels of specific chemicals in these tiny areas of the brain.]
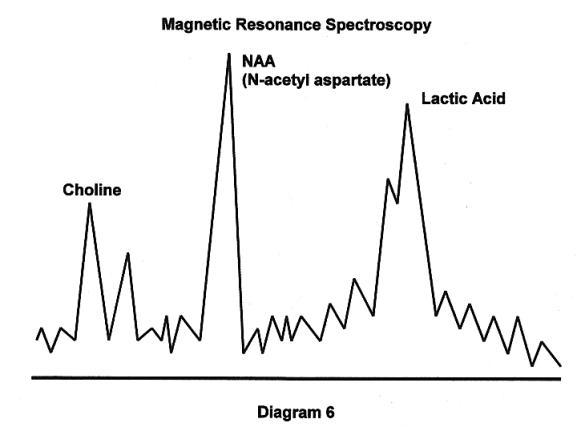
This is a spectroscopic scan of a single voxel on a CFIDS patient [each peak representing a different chemical], and I want you to see this big lactic acid peak right here. That lactic acid peak is definitely not normal. There should be no lactic acid peak in the central nervous system. It should be absolutely zero. So what is a large lactic acid peak doing in the brain? It means mitochondrial encephalopathy [brain cell dysfunction caused by mitochondrial dysfunction]. It means the brain isn't working because there isn't enough mitochondrial function to provide energy for it to work. You make lactic acid instead, and you get intracellular acidosis in the brain. The NAA [N-acetyl aspartate] peak is the viability peak. [Viability means ability to survive. NAA is an amino acid synthesized in the mitochondria and found almost exclusively in nerve cells; NAA levels drop after a nerve cell dies.] The choline peak examines in effect the cell membrane. [Choline is one of the chemicals found in the structural components of all human cell membranes.]
Magnetic Resonance Spectroscopy; N=20 [20 test subjects]
70% of patients show elevated lactate levels in the thalamus and surrounding structures.
10% of patients show reduced NAA peak and elevated choline peak, also in the thalamus and surrounding structures.
Recent studies out of the University of Liverpool show similar findings in the hippocampus of CFS patients.
We have used MRS to examine about 20 patients at Columbia Presbyterian Hospital in Manhattan. Seventy percent of patients show elevated lactic acid levels in the thalamus and surrounding structures, a subcortical area. Ten percent of patients show, in addition, reduced NAA peaks and elevated choline peaks, also in the thalamus and surrounding structures. A reduced NAA peak and an elevated choline peak represent potential cell death. They indicate the loss of neurons in that area, where the metabolic injury is so severe that you've actually lost the neuron itself. Recent studies published out of the University of Liverpool on MRS in CFIDS show similar findings in the hippocampus in CFIDS patients. The hippocampus is the area of short-term memory, particularly the right hippocampus.
The point is that we now have the capacity to probe very tiny areas within the brain and actually see this mitochondrial dysfunction, and beyond that even to see the repercussions of energy deficits and other problems that lead potentially to cell death within these small areas of the brain.
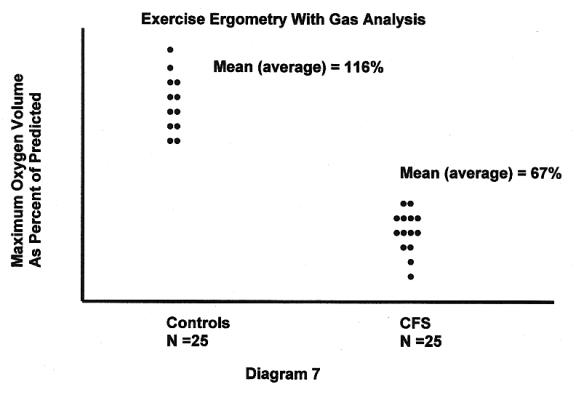
This is exercise ergometry [energy measurement] with gas analysis [which measures oxygen consumed and carbon dioxide produced]. This is 25 normal people picked by random digit dialling, age- and sex-matched with 25 disabled CFIDS patients. Both groups reached what's called end-point maximum on exercise bicycle ergometry [the point at which the body exhausts its aerobic capacity and switches back to anaerobic metabolism]. Notice the significantly lower levels of oxygen consumption at end-point for CFIDS patients compared to normal individuals, another indication that they're not consuming oxygen normally. We surmise that this is due to impaired mitochondrial function [since oxygen consumption is a measurement of the energy produced by mitochondria in aerobic metabolism].
PART II, TREATMENT
The Key Scientific Literature
|
Step I |
Holmes et al. (CDC) |
|
Bell et al. (Lyndonville, N.Y.) |
|
|
Rowe et al. (Johns Hopkins U) |
|
|
Step II |
Zivin et al. (Scientific American) |
|
Moorkens et al. (U Antwerp--Belgium) |
|
|
Cox et al. (The Lancet--U.K.) |
|
|
Step III |
Bland et al. (Healthcom, Inc.--U.S.A.) |
|
Step IV |
Beck et al. (New England Journal of Medicine) |
|
??? et al. (Karolinska Institute--Sweden) |
Now we're going to move into treatment. As I did with the scientific literature on pathophysiology, I want to go through some of the key scientific literature on treatment. There is the Holmes et al. article at the CDC, published in 1988, which says that one of the principal criteria for CFIDS is that exercise makes you worse. This is interesting given some of the recent articles in newspapers that say that exercise makes you better. But in reality, if you have mitochondrial dysfunction, exercise is contra-indicated, just as it is in mitochondrial cardiomyopathy. [Cardiomyopathy is a disease of the heart muscle.] Secondly, it's in the case definition that exercise makes you worse, so why would you think you should exercise, if it makes you worse? But we'll go through what type of exercise may be appropriate for CFIDS patients. It may simply be that different definitions of exercise might account for different recommendations.
Bell et al. looked at the blood volume issues. It's very important to address blood volume, but I think you need to do it adaptogenically since it's a compensatory issue. [Reduced blood volume is the body's attempt to compensate for a more basic problem. Adaptogenic therapies are designed to help the body adapt to various kinds of environmental, physiological, and psychological stress.]
Rowe et al. out of Johns Hopkins identified tilt-table positivity, which is essentially a subset of patients with blood volume depletion. [The tilt-table test measures orthostatic intolerance or neurally-mediated hypotension, which are associated with weakness or fainting when standing, even for short periods.]
Zivin, publishing in Scientific American, has talked about the importance of NMDA-receptor-mediated neurotoxicity and the extreme importance of blocking that receptor or agonizing its opposite, to protect the brain against injury of any kind. [This subject is discussed in detail later in the summary.]
Moorkens' work, particularly on the importance of magnesium in treatment, would fit very well with Zivins' article, since magnesium is an NMDA receptor blocker.
Cox did a magnesium study, a double-blind placebo-controlled study, showing that magnesium was beneficial in CFIDS.
Bland has done the most work in detoxification, using nutritional approaches to resuscitate liver function, which have shown benefit in CFIDS in a multi-center trial.
Beck, publishing in the New England Journal, and a Swedish person whose name I don't remember--I did this on the plane coming in, so I don't remember his name--publishing out of the Karolinska Institute in Stockholm, both showed that CFIDS patients have low vitamin B-12 levels in their brains but normal levels in the blood. They also have elevated homocysteine in the brain, but normal levels in the blood, suggesting that there's a B-12 deficiency in the brain, not present in the blood, that needs to be very aggressively addressed, because the brain doesn't work very well without B-12. [Homocysteine is an amino acid formed during the metabolism of the essential amino acid methionine. High levels of homocysteine in the blood are caused by deficiencies of folic acid, B-6 and B-12 and may contribute to atherosclerosis and heart disease. The presence of homocysteine in the brain is evidence of B-12 deficiency.] If you don't address B-12 deficiency, you get problems with lack of S-adenosylmethionine function and you also get problems with homocysteine action. [S-adenosylmethionine, which is marketed as the nutritional supplement SAM-e, is also produced by the body in the process of metabolizing methionine, but its effects are positive. SAM-e is found in every cell in the body, and is involved in more then 100 important chemical reactions. It is a donor of methyl groups, specific chemicals necessary for the formation, activation, or metabolism of many essential substances, including glutathione, neurotransmitters, hormones, and proteins.] The B-12 deficiency doesn't show in the blood, but this article shows that you have to treat it. I think eight out of 10 patients had B-12 deficiencies in the brain.
The Key Scientific Literature
|
Step V |
Pimental et al. (UCLA) |
|
Haley, Boyd et al. (U Kentucky) |
|
|
Ray et al. (Dallas, Tex.) |
|
|
Step VI |
Bland, et al. (Healthcom, Inc. -- U.S.A.) |
|
Bennett, et al. (U. Oregon) |
|
|
Moorknes et al. (U Antwerp -- Belgium) |
|
|
Misc. |
Carter et al. (Hemispherx, Inc. -- U.S.A.) |
|
Ablashi et al. (NIH) |
|
|
Berg et al. (Hemex, Inc. -- U.S.A.) |
Pimental--that is the U.C.L.A. group that used antibiotics to treat the gut. Patients got better, showing that gut resuscitation, gut ecology manipulation, can be important to treat this disease. Boyd Haley's group at the University of Kentucky has done most of the really good scientific work on mercury issues as they may pertain not only to CFIDS but to the broader population. Ray's group, I believe here in the Dallas-Fort Worth area, has done as much as anybody to point out that environmental illness makes people sick, and of course environmental issues could affect some of our patients. Bland also has done a lot of work in the area of detoxification procedures and published several articles in nutrition journals. Bennett and Moorkens have been doing work in growth hormone. Bennett did a double-blind, placebo-controlled trial that showed growth hormone was of benefit in fibromyalgia. Moorkens did growth hormone studies in CFIDS that showed a partial benefit in some patients and no benefit in others, but her dose was very high. We'll talk about dosing with growth hormone and how important that is. Then some miscellaneous publications. Carter wrote the article on Ampligen for regulating RNase-L. There's the Ablashi article showing that Kutapressin inhibits all known human herpes viruses in a test tube. [Kutapressin is a drug made from pig liver extract. It is a broad-spectrum anti-viral, and Dr. Cheney has used it in patients who test positive for viruses such as EBV, CMV, and HHV-6, all herpes viruses.] And then the Berg article out of Hemex which brings into focus the coagulopathies [abnormal presence of substances involved in blood clotting] associated with immune activation that plague perhaps 40% to 50% of CFIDS, suggesting the use of anticoagulant [clot-preventing] therapies.
Treatment Overview
Phase I--High RNase-L Activity/TH2 Activation With or Without Coagulopathy [abnormal presence of substances involved in blood clotting]
Ampligen
Anti-microbial Therapy (Quantitative PCR Testing Now Available)
Immune Modulation (TH2--TH1 Shift)
Anticoagulant Therapy
How do we treat Phase I, which involves high RNase-L, TH2 activation, with or without coagulopathy and also involves, to some extent, microbial infection? Active microbial infection would fit into the Phase I pattern. One of the best regulators of RNase-L ever is the double-stranded RNA molecule known as Ampligen. And I think it does have a role, will have a role, particularly in those individuals with what might be called inappropriate upregulation of RNase-L, perhaps with the low molecular weight variety, which seems to be unregulated. I don't know what exact percentage of patients have that, but based upon clinical observation, it seems maybe 50% or so, maybe slightly less than 50% might expect to respond to Ampligen.
Anti-microbial therapy obviously could be important, particularly with appropriate RNase-L activation because of an active infection of intracellular microbes, particularly viruses, and also intracellular bacteria, Mycoplasma or Chlamydia pneumoniae, for example. We have a new technology that has just become available a few months ago. It's call a Taqman assay [measurement], and it's otherwise known as a fluorescent tagged, triple-probed PCR technology, which can measure actual quantities of the virion. [PCR testing involves the polymerase chain reaction, which can produce many copies of a DNA fragment. This increases minute traces to levels more easily detected. Fluorescent tagging is a method of using fluorescent dyes that show up under the microscope. A virion is a single mature virus.] It's an antigen detection device. [An antigen is any substance that can cause an immune reaction. Antigens are found on the surfaces of microbes and are identified by the immune system as foreign substances.] It detects the virus or the Mycoplasma or the Chlamydia itself with great precision. It can actually measure the quantities of microbes in ccs. [cubic centimeters] of blood, typically ccs. of plasma or serum [the liquid left after blood cells have been removed]. Testing the serum avoids false positives you might get by testing for microbes in the blood cells. [A false positive reading would indicate an infection when no infection is actually present.] You could have dormant herpes group viruses, even dormant Mycoplasma or Chlamydia which would show positive if you test the blood cells but don't really contribute to an active infection.
Because you don't have to worry as much about false positives with this method, you can really ramp up [increase] the sensitivity rate and you can even measure a single virion per cc. of blood. This assay is expressed in things like 58,000 copies of HHV-6 strain A per cc. of serum. Or 30,000 copies of Epstein-Barr virus per cc. of serum. Or 28,00 copies of CMV per cc. of serum. As of January of this year, they're going to be offering this Taqman assay for all Mycoplasma species and Chlamydia pneumoniae, which will offer us the ability to look not only at herpes group viruses but also at some of these intracellular bacteria. I think this will be a tremendous advance in being able to single out those individuals who may have an active microbial infection and may need specific therapy for that. So far, we've done about 50 assays on HHV 4, 5, 6, and 7. HHV-4 is Epstein-Barr, HHV-5 is cytomegalovirus, HHV-6 is HHV-6, and then HHV-7 is similar to six. So far it's running about 40% positive in my patient population, which really surprised me. I had no idea that high a percentage would have an active viral replication rate [an active infection] going on in their blood.
How would you treat an active viral infection? There are many ways to go here, and I've tended to use a mix of immunomodulation methods that tend to augment TH1 [the part of the immune system that fights viruses] and also specific anti-viral measures. But since the Taqman assay measures specific amounts of viruses, you get feedback. Whatever treatment you choose, you simply test again to see if the number of viruses is coming down. If it's coming down, whatever you're doing is working. If it isn't coming down, it isn't working. So you just try something you think might work, and you get reliable feedback, and it's relatively inexpensive to do repeat testing for a single microbe.
QUESTION: How much does it cost to do the Taqman assay?
The panel of four viruses, HHV 4, 5, 6, and 7, is about $550. The individual assays are about $180. So once you get a positive, and then you're testing a single one repeatedly to see if the treatment is working, you're only paying $180 per test.
Immune modulation is the concept of augmenting the immune system that fights intracellular microbes; that's the TH1 system. There are a number of pharmaceuticals and nutriceuticals [nutritional supplements used therapeutically] that do that. The one I like the best is isoprinosine, a drug that unfortunately is not approved in this country but is approved in 51 other countries, made in Dublin, Ireland, by Rivex Pharmaceuticals, although discovered in this country.
We have probably a couple of hundred people on isoprinosine. It's the only immunomodulator I've ever given where people actually call us back and tell us how much better they're doing. I've never had an immunomodulator that strong before. Kutapressin wasn't nearly that strong. Isonisoprine is relatively safe and relatively inexpensive. [Although isoprinosine (brand name Immunovir) is not approved in the U.S., Dr. Cheney sends a prescription to the Canadian supplier, which ships the drug to the patient. Some patients also obtain the drug directly from the manufacturer in Ireland.]
Anti-coagulant therapy. Those individuals who are forming soluble fibrin monomer [SFM] or whose immune coagulation pathway is really turned on may need, at least for a time, anticoagulant therapy. [The theory proposed in the Hemex article is that pathogens like CMV, HHV-6, Mycoplasma incognita, and Chlamydia pneumoniae, and the body's immune response to them, alter cell chemistry in ways that lead to the production of SFM and other substances involved in the blood clotting process. These substances make the blood cells cling together, which can reduce the efficiency of blood flow, especially in the smallest blood vessels.] We typically use heparin and treat for maybe three to six months. Then we may stop, because once you address the immune activation state that causes the coagulopathy, often the coagulopathy will downregulate [return to normal], and you don't need to treat it any more. I think this year or next year they're going to be coming out with oral heparin, so heparin will go from an injectable to oral tablets, which will be easier. [Heparin is an anticoagulant that occurs naturally in the tissues and is also used in medicine. It inhibits the enzymes responsible for blood clotting.]
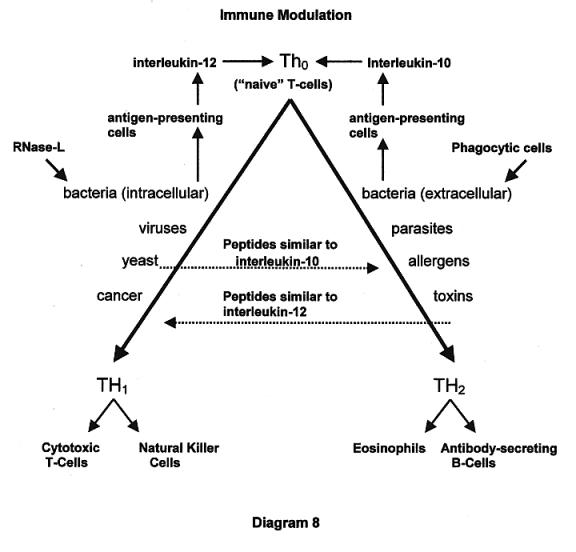
Carol [Sieverling of the Dallas-Fort Worth Support Group] made a diagram of this TH1-TH2 system that's really nice; it shows how antigen-presenting cells upon receipt of a certain antigenic stimulus, tell naïve TH cells to either go down the TH1 system or the TH2 system. ["Naïve" TH cells are undifferentiated; they have the ability to become either TH1 or TH2 cells.] Antigen-presenting cells, that is macrophages, swallow whole the micro-organism or its antigenic component and then send out cytokine information to the naïve T cell. [Cytokines are the immune system's chemical messengers.] Depending on the cytokine [interleukin-10 or interleukin-12], that either forces the cell down more the TH1 pathway or forces it down more the TH2. Often it gets forced down both pathways, but there will usually be a dominant one. The effector cells [cells that actually fight the infection] for TH1 are cytotoxic [cell-killing] T-cells and NK [natural killer] cells. The effector cells for TH2 are antibody-secreting B-cells and eosinophils. [Cytotoxic T-cells recognize antigens on the surface of cells infected by viruses and release proteins that kill the cells. Natural killer cells are lymphocytes (a type of white blood cell) that are able to kill virus-infected cells and some types of cancer cells. Eosinophils are leucocytes (a type of white blood cell) involved in allergic reactions; they also produce an enzyme that can destroy parasites. B-cells are lymphocytes with receptors that detect specific types of antigens. When the receptors detect these antigens, the B-cells divide and produce large amounts of antibodies to the antigen.]
One interesting difference between these two systems is that the TH1 system kills human cells that are either infected with something or are abnormal, like a cancer cell. They kill specifically human cells. Conversely, the TH2 system tends to kill organisms outside the human cell. The kinds of antigens that force cells down the TH1 system are viruses, cancer, intracellular bacteria, and yeast, and all of these seem understandable from an intracellular perspective, except yeast. Yeast really isn't an intracellular microbe. I think the body perceives yeast as a kind of cancer cell or some sort of human cell that has gone wrong. For some reason, yeast is stuck over on the TH1 side. Conversely, extracellular bacteria, allergens, toxins, and parasites tend to initiate more of a TH2-type response.
RNase-L is holding the line on intracellular replication rates, waiting for TH1 to arrive in the form of cytotoxic T-cells or NK cells. [RNase-L can't eradicate a viral infection; it only reduces the virus's reproduction rate until the TH1 system gears up to knock out the infection.] Here's the problem in CFIDS patients: If TH1 is downregulated, which it is, then RNase-L simply stays activated, waiting for the TH1 cavalry to arrive, and it never arrives. Therefore, one of the factors keeping RNase-L upregulated is the loss of the TH1 system. TH1 is the only thing that can actually eradicate the microbe; all RNase-L will do is inhibit its replication rate.
Over here, on the TH2 side, the phagocytic cell, particularly the granulocyte, typically is what is fighting some of these things, waiting for the TH2 system to arrive. [Phagocytic cells can engulf and digest microbes. Granulocytes are phagocytic white blood cells.] These two cytokines--interleukin-10 tends to move one from the TH1 system to the TH2 system. Interleukin-12 tends to move you from the TH2 system to the TH1 system. Here's where it gets interesting. Viruses, one example being the Epstein-Barr virus, have DNA that allow them to make protein similar to interleukin-10. Now why would a virus be spitting out an IL-10 like protein? Well, look at the advantage to that virus. If it can make IL-10, it will shift the immune system away from fighting viruses, so the immune system won't kill this virus. The virus is capable of altering the immune system away from itself by virtue of its capacity to make an IL-10-like molecule. It has been discovered that parasites make an IL-12-like molecule, and parasites will shift the system toward TH1, and therefore the parasite doesn't get killed. The point is, these microbes have some intelligence, as it were, or they're mutating in directions that allow them to survive our immune system. They do that by making proteins that mimic our cytokines and actually shift our immune systems away from themselves. That can explain some of the vagaries [unpredictable factors] you can get into and why some of these viruses can be so difficult to eradicate, if they're actually altering the immune system that otherwise would get rid of them.
Treatment Overview, Phase II--Xenobiotic Toxicity
Source Attenuation [reduction]
gut
teeth/jawbone
environment
High Dose Hydroxycobalamin
MSM [methylsulfonylmethane]
Whey Protein Concentrate
Guaifenesin
Growth Hormone
Treatment overview for xenobiotic toxicity. First we deal with toxin source attenuation; we reduce the gut source; we reduce the teeth and jawbone source; we reduce the environment source. You notice I say "attenuate;" I didn't say "eliminate." In fact, there's no way to get rid of a toxic gut; there's no way to get rid of a toxic mouth, and there's no way to get rid of a toxic environment, but you can reduce the most serious types of toxicity.
Then you engage in first-order detoxification. Hydroxycobalamin is a form of B-12 that acts as a potent central nervous system detoxifier. [Doses are discussed later in the summary.] In fact, it's kept in emergency rooms to detoxify cyanide. It's an excellent antidote to cyanide poisoning, but it actually is an excellent antidote to any nitrogen-bearing toxin, and most fat-soluble toxins from the gut [which tend to concentrate in the brain], interestingly, are nitrogen-bearing. So B-12 could be excellent as a nonspecific brain detoxifier [effective against many toxins]. And I think the reason why it's depleted in the brain is because it's being complexed out faster than it's being replaced [bonding with toxins and being eliminated along with them].
MSM--wonderful nonspecific detoxifier. The sulfur group on the MSM binds to a lot of different toxins and can remove them. There's quite a bit of literature on the use of MSM to treat pain, at least the toxic component of pain, and it is a pretty good detoxifier, even for heavy metals.
The problem that you get into particularly with MSM, but also with all of these, is that you can overmobilize when you over-detoxify. [The first step in the detoxification process is to pull toxins out of the tissues where they have been stored. If toxins are pulled out of the tissues faster than they can be neutralized, they are mobilized--allowed to move around the body and cause damage.] By that I mean, what detoxifies also mobilizes, and if you mobilize more than you can handle, you can actually get sick. So we've seen people take high doses of B-12 and break out in acne-form eruptions all over their face and body as the toxins actually come through the oil glands of their skin. [Diarrhea, acne, lethargy, agitation, and increased insomnia are signs that the toxins are being mobilized faster than the body can eliminate them, and the dose should be reduced.] We've seen people start on high doses of MSM and get extremely ill. [Dr. Cheney recommends starting with a very low dose and increasing it very slowly up to the therapeutic dose, which is 6 to 9 mg. a day. Pain relief can be significant at that level. MSM is effective against yeast and can also help with allergies. The sulfur bonds to allergens, and keeps them away from the mucous membranes in the nose and sinuses. MSM is available from the CFIDS and Fibromyalgia Health Resource, 800-366-6056, www.immunesupport.com and from www.needs.com]
QUESTION: Will MSM bind to nutritional supplements and make them ineffective?
Possibly. I would worry particularly about minerals. Sulfur would bind minerals pretty well. So I wouldn't take MSM at the same time as a multivitamin or a mineral supplement. Otherwise, I wouldn't be particularly worried.
We've seen people intolerant of whey protein concentrate, which raises glutathione concentrations in the cell and can also overmobilize toxins. [Glutathione is a powerful detoxifier, and Dr. Cheney believes whey protein concentrates are the most effective means of increasing glutathione levels, which also increases energy production in the mitochondria. Whey proteins can also reduce levels of Mycoplasma incognitus and Chlamydia pneumoniae. Some of Dr. Cheney's patients had dramatic improvements after a few months on whey protein concentrates. Whey is the watery part of milk that is left after cheese-making. However, these whey proteins are not the result of cheese-making; they are extracted by a different process. The most effective whey proteins are those that are very weakly denatured and then stabilized. "Denatured" means broken down into the constituent amino acids. So weakly-denatured proteins are slightly broken down.
[Dr. Cheney tested Immunocal, the first undenatured whey protein to come on the market, and has great confidence in it. Another product that seems to be very similar is ImuPlus. A slightly different product, ImmunePro, seems to be very powerful; in fact, it may mobilize toxins faster than the body can eliminate them. Some people are using Immunocal or ImuPlus as their primary whey protein, and taking small doses (1/4 teaspoon up to 1 or 2 teaspoons) of ImmunePro every second or third day. All three of these products are available from the CFIDS and Fibromyalgia Health Resource, 800-366-6056, www.immunesupport.com]
Guaifenesin is famous for causing toxic reactions. [Guaifenesin is a drug often added to cough syrups to loosen mucus. It is available by prescription in higher concentrations. Some CFIDS and fibromyalgia patients have found it effective in reducing pain. However, the effects of guaifenesin are counteracted by salicylates, a large class of compounds including aspirin. Its effects are also counteracted by many herbs. Therefore, patients taking guaifenesin must be extremely careful to avoid using any of these compounds, and they must take guaifenesin for several weeks before they begin to feel a improvement.]
And even growth hormone, which may be the best detoxifier of them all, since it increases protein synthesis in the liver and improves liver detoxification, may actually produce a variety of toxic reactions, particularly at pharmacologic and possibly even physiologic doses. [A physiologic dose is an amount approximating what the body would produce under normal conditions. A pharmacological dose increases blood levels many times higher than they would normally be.] So you have to be really cautious with the doses of these detoxifiers, or you can really get into trouble. If you get into trouble, you just cut the dose in half, and usually you're out of trouble pretty quickly. You start the detoxifiers one at a time, and you go carefully. And some are worse than others [in terms of mobilization and toxic reactions]. MSM is probably the worst of the bunch. And growth hormone can be pretty bad if you take a physiologic dose.
Treatment Overview, Phase III--CNS [Central Nervous System] Injury/DNA Damage
Growth Hormone Stimulation
Secretagogue Therapy--limited
GH Injections, low dose
Fetal Bovine Growth Factors--limited
Mesenchyme/Liver
Thymus/Adrenal
Central Nervous System
How do you treat the brain? How do you treat the hypothalamic injury? And there we thought about trying what a lot of neuroscientists are now trying, stem cell research and growth factor research, especially for Parkinson's Disease and other conditions such as spinal cord injury, to actually resuscitate and repair lost neurons. We thought the same might be done with CFIDS patients, and so we've had a study; it's about a year old now. We're studying both growth hormone therapy and growth factor therapy. The idea is to heal the brain and heal the body, using the primary methods by which we heal, namely stem cells, growth factor. and growth hormone.
[Growth factors are chemicals, particularly polypeptides, that have important roles in the stimulation of new cell growth and cell maintenance. Specific growth factors can cause production of new cells and play a role in wound healing. It is thought that growth factors that induce cell production can increase the growth of tumors.
[Growth hormone secretagogues are formulations intended to increase growth hormone production. They include all the amino acids the body needs to produce growth hormone and may include other substances intended to protect the amino acids from being damaged by the digestive system.]
Initial Treatment of CFS--Principles
Integrated program (No one element suffices.)
Stepwise (Move to next step every 2 weeks as tolerated)
Patience is required (8 months typical)
Failure in some patients
High 37 kda RNase-L activity (Phase I Illness)
Non-compliance
Treatment principles. It's an integrated program; no one element suffices. It's a stepwise program; we always start with one step and move up progressively, making a move every two weeks. The importance of that is to identify responses to any given step and also identify problems with any given step, because that always gives us information about the illness. Patience is required; it can take eight months before one knows really how well this program might work. Failure does occur, and these are some of the reasons for failure. Those with high 37 kda unregulated RNase-L activity will typically not benefit from this program, because they have an unregulated, disregulated RNase-L system, and nothing in here, short of Ampligen, is likely to affect that. [37 kda RNase-L is the more destructive, low molecular weight, variety.] Noncompliance--they either won't do what we say or they cannot do what we say.
Sometimes failure occurs because I missed something, and what that really means is that I put it on a back burner and hoped it wasn't a problem. The one I usually put on a back burner is root canal teeth. I usually make the initial assumption that root canal teeth are not a problem. I usually also make the initial assumption that mercury is not a problem, and I usually make several other assumptions about the environment and hope it is not a problem. Oftentimes, if you get failure, it's because the things you thought were not a problem were the exact problem they were having. So sometimes you have to revisit those when failure occurs.
Sometimes failure occurs because it's not time yet. This illness is like a great ship with a certain momentum, and it turns and moves at its own rate. It seems to me that sometimes people get better in their own time, and I don't know that the treatments we have are powerful enough to change that. And finally, some people are pretty much through the illness; they're in Phase III, and they really need, I think, brain resuscitation as their primary focus.
Treatment--Step I, Lifestyle Adjustments
Limit Setting
Oligo-Antigenic Diet
Digestive enzyme support
Betaine HCL support (careful)
Exercise Prescription
Anaerobic and rebound exercise
Limit aerobic exercise to tolerance
Step I. Set limits, because the disturbances of dynamic hormone response demand that patients set limits, and they have mitochondrial dysfunction that demands limit-setting as well. But that doesn't mean you crawl in bed and pull the covers over your head and retreat, because then that circle of dysfunction closes in on you. What you do is go out and meet it and sort of shake hands with your limits, so you know where they are. And don't be afraid to occasionally cross the limit and get punished for doing that, because sometimes that's the only way you know where the limit is. Crossing limits occasionally is not a devastating thing. It isn't permanent damage that you're doing; it's just your body letting you know where the limit is. The problem occurs when people consistently cross the limit believing that if they do that they'll get better. They don't. They get worse.
[Dr. Cheney has said that patients need to start defining themselves in terms of who they are rather than what they do. He says that patients often begin to improve when they make the shift away from doing and recovery and toward being and healing.]
Oligo-antigenic diet is very important in about 10% of patients, moderately important in another 40% of patients, and seems to be not important in about half the patients. [An oligo-antigenic diet is designed to reduce or eliminate foods that cause allergic reactions.] So we use a type of food testing called Alcat technology, which allows us to look at all four types of immune reactions, Type I, Type II, Type III, Type IV, whereas most immune system tests only detect one type. Then we try to eliminate the foods that are causing problems. One little caveat [warning] about food testing: all food testing has a great number of false positives and false negatives, and it changes over time, so it is never an exact test. You must always be alert to that. A false positive is an indication of an allergic reaction where there is in fact no allergy. A false negative indicates no allergy when in fact there is an allergy.
[Dr. Cheney also makes the following diet recommendations:
[Avoid sugar. It produces toxins (free radicals) that can cause pain, headaches, and neuropsychiatric problems. It stimulates growth of abnormal gut microflora, especially Candida albicans (yeast), and it raises insulin levels, which can cause blood sugar levels to drop sharply and increase fatigue. If you crave sugar, try eating other carbohydrates instead. If you do eat sugar, including fruit, it should be with meals, never alone. Honey and powdered fructose can be used in cooking, and the herb stevia can also be used. (Stevia is a noncaloric herb, native to Paraguay, that is extremely sweet and has been used as a sweetener for centuries. It is sold in various forms in health food stores.)
[No NutraSweet. It contains methanol, a toxin, and can increase neurotoxicity.
[Limit daily fat intake to 30 grams, and avoid saturated fat. Essential fatty acid supplements are necessary. (Doses are given later in the summary.)
[No caffeine--or at least limit it as much as possible.
[Avoid red meat. It has a lot of saturated fat and is difficult to digest. It can cause GI tract symptoms and systemic symptoms such as joint pain.
[Dairy products and gluten (found in wheat and oats and therefore in cereal, bread, and pasta) can cause GI tract and systemic symptoms. Eliminate them completely or use an elimination diet to see if symptoms improve while you're not eating them. Gluten-free foods are available.]
Another important thing is to digest well. We use digestive enzyme support and always add acid. I think adding acid is more important than it seems, because you remember I said the cells are acidic, but the extracellular environment is alkaline. The result is that the stomach is not as acidic as it used to be, and that is the cause, I believe, of the small bowel bacterial overgrowth seen in 92% of patients in the UCLA breath hydrogen study. In fact, if you read the medical textbooks, the most common cause of small bowel bacterial overgrowth is hypochlorhydria [reduced stomach acid] or achlorhydria [absence of stomach acid]. And the problem with hypochlorhydria or achlorhydria is that digestive enzymes in the stomach do not work well if acid levels are too low. Secondly, and you may be surprised to hear this, one of the most common symptoms of too little stomach acid is reflux esophagitis [irritation of the esophagus, caused by reflux or backward flow of stomach acid]. That is kind a contradiction, because people would think, doesn't that mean you have too much acid? No, it actually means you have too little acid. When you have too much acid, you get duodenitis and duodenal peptic ulcer disease. [Duodenitis and duodenal ulcers are irritation of the duodenum, the first part of the small intestine.] If you have too much acid, you burn the area of outflow from the stomach, and if you have too little acid, you burn the area of inflow [the esophagus]. It has to do with the way the stomach deals with acid changes and the way the pyloric valve functions. [The pyloric valve is the opening from the stomach to the duodenum. When food enters the stomach, the stomach produces acid to aid digestion. When there is sufficient acid, the pyloric valve opens and releases the partially digested food into the small intestine. If there isn't enough acid, the valve doesn't open, and food and stomach acid can be forced back up the esophagus.
[Dr Cheney believes stomach acid has four important functions: (1) Acid helps kill bacteria in the stomach, which prevents bacterial overgrowth in the small intestine. (2) Acid breaks down proteins, which begins the protein digestion process. (3) Acid helps extract minerals from food, so they can be absorbed by the body. (4) When the partially digested food enters the small intestine, normal acid levels must be present to trigger the release of pancreatic enzymes and bile, both essential for good digestion.
[Dr. Cheney believes most CFIDS/FMS patients need supplemental betaine hydrochloride, a form of hydrochloric acid, to provide necessary stomach acid levels. He recommends Betaine Plus, made by Douglas Labs. It is available from NEEDS, 1-800-634-1380, www.needs.com Dr. Cheney recommends as much betaine as the patient can tolerate, and they have to experiment to find the right dose. This ranges from half of a 500-mg. tablet with each meal up to seven tablets. If you take too little, you can still have problems with acid reflux. If you take more, but still not enough to trigger the opening of the pyloric valve, you will still get acid reflux, but the burning will be worse because acid levels are higher. If you take too much, you can get diarrhea or just feel generally bad. You should not take betaine if you have a duodenal ulcer.]
Exercise prescription. Anaerobic exercise is well-tolerated. [Anaerobic exercise is weight-lifting up to 20 pounds, stretching, or isometric exercise. Dr. Cheney recommends that the exercise be limited to 10 seconds, followed by 60 seconds of rest before the next lift or stretch. This should be continued for not more than 20 minutes not more than three times a week.]
Rebound exercise is probably the very best exercise to do. We like the rebound chair, made in California. It's a chair on bungee cords in a metal frame. You just bounce. [The Bounce Back Chair is available from Sun-Ray Supply, 800-437-1765.] It comes in a box, and you can have it up in a couple of hours. I think its base is about three feet square. It has been used by NASA; they use it to resuscitate astronauts who return from space very de-conditioned. Their autonomic nervous systems aren't working properly, and rebounding brings them back quite readily. [The autonomic nervous system controls such basic processes as functioning of glands, heart muscle, and the muscles of the digestive system. The up and down motion improves autonomic functioning and also improves immune function by increasing the flow of lymph fluid.] It's very easy for CFIDS patients to engage in. You can just bounce to improve autonomic nervous system functioning, or you can use your arms and legs for a little aerobic activity. [Low-level non-vigorous bouncing for 10 to 15 minutes every other day is recommended. The videotape that comes with the chair shows how less ill patients can add short periods of aerobic exercise. Rebounding is the most efficient exercise for CFIDS patients; it brings the greatest benefit with the least expenditure of energy. Those who do not have balance problems can achieve many of the same benefits from bouncing gently on a mini-trampoline.]
Be careful with aerobic exercise, and try not to pass the limits and induce relapses. It's okay to do as much aerobic exercise as you can tolerate, but do not exceed that tolerance. So if you can play to your strength, which is the anaerobic system; be aware of your weakness, which is the aerobic system; and then use rebounding--which is probably the most efficient exercise system for this disease--then you're probably exercising correctly.
Treatment--Step I, General Metabolic Support
Blood Volume Adaptogenic Expansion
Gookinaid ERG/Isotonic Home Recipe
Oxygen Transport
Daily Breath Holding Exercises
Diamox L.A. [long-acting] 500 mg. daily
Autonomic Nervous System Regulation
Rebound exercises
Body work
Expansion of blood volume. We use an isotonic drink called Gookinaid; there's also an isotonic home recipe, which is Gookinaid without the sugar, that you can mix yourself. [Gookinaid E.R.G. (electrolyte replacement with glucose) is an electrolyte replacement solution that Dr. Cheney says may be the most isotonic mixture (chemically similar to body fluids) he has seen. Electrolyte drinks were developed to replace water and minerals lost when you are fatigued. Dr. Cheney says that most patients can drink Gookinaid without problems. Even those who are glucose-intolerant rarely had problems with Gookinaid as long as they sipped it slowly. The only problems his patients reported came from "chugging" it rather than sipping. Gookinaid is available at 1-800-283-6505 or http://members.aol.com/Gookinaid and is also sold by outdoor supply companies like Campmor, 1-800-226-7667. A 1.8-oz. packet, enough to make one quart, is $.99. A 1-kilo tub, enough for 19 quarts, is $11.00. In case you're wondering why anybody would name something Gookinaid, the product developer and company owner is named Bill Gookin.
[The recipe for the home-made substitute is: 1 C. spring water, 1 C. seltzer water, ¼ tsp. sea salt, and ¼ tsp. "No Salt" salt substitute (potassium). Adding stevia and an herbal tea bag can improve the taste. Sip over ice. Dr. Cheney recommends three or four glasses a day. Monitor your blood pressure response. Consider stopping if your blood pressure rises above 140/90.]
Essentially, isotonic drinks expand blood volume adaptogenically, which means that if your body truly needs to a low blood volume [to compensate for other problems], you'll still be able to have it. On the other hand, Florinef will increase blood volume whether that improves your over-all condition or not.
Oxygen transport. We use daily breath-holding exercises developed 3,000 years ago by Ayurvedic physicians and in the present day promulgated by Andrew Weill in his breathing tape, "Breathing, the Master Key to Self-Healing." It's a series of breath-holding techniques that essentially tricks the body into thinking it's at high altitude, and you get increased 2,3 DPG in the red cell to improve oxygen transfer. [Ayurvedic medicine is the traditional holistic medicine of India and Sri Lanka. The word "Ayurvedic" comes from the Sanskrit "ayur," which means "life;" and "veda," which means "knowledge."]
QUESTION: Please repeat the title and purchase information for the book regarding daily breath-holding exercises.
That is Andrew Weil's CD and tape. He offers eight breathing exercises, and the eighth one he describes is the one we recommend. [Inhale through your nose for four seconds. Hold your breath for seven seconds. Exhale through tightly pursed lips for eight seconds, creating back-pressure. You should be able to hear the air being forced out of your mouth. Do this eight times in a row, twice a day. If you feel light-headed, just do it six times, or until you begin to feel light-headed, and then build up to eight times.] It takes two and a half minutes twice a day. If you're only breathing for four seconds, and you're not breathing for 15 seconds, eight times in a row, you're getting a progressive loss of oxygen in the blood, and the body interprets that as a rise in altitude. And the body starts generating 2,3 DPG. Weil and others have shown that it takes several weeks to several months to get a 2,3 DPG shift. You can detect the 2,3 DPG shift yourself very simply; if red-cell 2,3 DPG is increasing, that breath-holding will get easier and easier and easier.
Diamox (acetazolamide) inhibits carbonic anhydrase and acidifies the blood mildly and promotes significant oxygen transfer. [Carbonic anhydrase is an enzyme involved in controlling the acid-base balance of the blood through formation of carbonic acid or bicarbonate.] It doesn't seem to increase acidity in the cell, because the cell's primary buffer system is the phosphate buffer system, whereas the primary buffer system in the blood is the bicarbonate buffer system that Diamox affects. We give the long-acting form, 500 mg. daily or twice a day.
Autonomic nervous system regulation. Rebound exercise is absolutely excellent. And body work, all kinds of body work, improves autonomic nervous system functioning. Massage therapy, acupuncture, acupressure, reflexology, cranial-sacral therapy, they all help the autonomic system, which is disturbed in this illness. [Cranial-sacral therapy is a form of very gentle massage, hardly more than touching and stroking, of the face and head, intended to release tension held in the neck and the skull. Reflexology is a form of foot massage intended to benefit the whole body. It is based on the theory that every part of the sole of the foot corresponds with an organ or part of the body, and massaging that area of the foot will benefit the corresponding part of the body.]
Treatment--Step I, Other Paths to Advance Self Healing
Autonomic Balance/ Stress Reduction
Conscious Beliefs and Attitudes (CBT/Siegel)
The Unconscious Wound (Imago Therapy)
The Transpersonal Self (Spiritual)
Other paths to self healing. I don't hit this too hard, because these are areas that I don't know a whole lot about, but I get feedback from patients enough to know that there's a wider world of healing than anything that I know that seems to work in some patients as well. It includes autonomic balance and stress reduction, perhaps through acupuncture. It includes conscious beliefs and attitudes such as Bernie Siegel's mind-body work and more formalized in cognitive behavioral therapy. [Bernie Siegal, M.D., is a cancer surgeon and the author of Love, Medicine, and Miracles and other books on mind-body interaction to promote healing. Cognitive behavior therapy has bad connotations for some patients, because doctors and others who don't believe in CFIDS promote "cognitive behavior therapy" to convince the patient that he or she isn't really sick. However, in its positive forms, it means understanding that there are things you can do to improve your condition and that you can live a better life in spite of being ill by learning better coping methods.] The Unconscious Wound and Imago Therapy is a rich area of psychodynamic that might improve the health of some people, especially when they have deep unconscious wounds such as childhood abuse. [Imago Relationship Therapy is a complex theory of therapy aimed at understanding how childhood psychological trauma may affect people in their adult lives. For information on the Institute for Imago Relationship Therapy, go to http://www.imagotherapy.com/about.html] And the transpersonal self or spiritual domain has long been known to be a healing domain for thousands of years, and so who am I to say that any one of these might not be of benefit to individuals who feel good about trying them. I encourage people to explore these more ancient healing domains.
Treatment--Step II, Neuroprotection via Threshold Potentials
NMDA Blockers [A blocker blocks a cell receptor site so the chemical messenger that normally acts at that site cannot reach it and has no effect.]
Parenteral [injected] Magnesium and Taurine
Histamine Blockers--Doxepin Elixir [a tricyclic antidepressant; brand name, Sinequan. The elixir is the liquid form, which can be measured out drop by drop.]
GABA Agonists [An agonist is a drug or chemical that acts at a cell receptor site to produce the same effect as the chemical messenger that normally acts at that site. So GABA agonists are chemicals that can produce the same effect in brain cells as GABA itself.]
Klonopin (Day and Night) [Klonopin is a benzodiazepine (the same class of drugs as Valium) used to prevent seizures in children.]
Neurontin (Night or Day and Night) [Neurontin is a drug used to prevent seizures.]
GABA (500 mg.-1500 mg./Night)
Valerian Root (Night) [an herb traditionally used to improve sleep]
Neuroprotection via threshold potentials. This is a very powerful treatment modality. It comes from my reading of Zivin's article in Scientific American. Actually, if you get Scientific American and you read it for the past ten years, about every third issue there's an article on this view of the nervous system actually running on a threshold potential, set by the balance between these two receptors or receptors similar to these two, the NMDA receptor and the GABA receptor.
[When neurons "fire" or transmit an impulse, a tiny electrical signal passes from cell to cell. The axons and dendrites or extended arms of the neurons don't actually touch; there is a very small space between. Neurotransmitters are chemicals that transmit the nerve impulse across the gap. The neurotransmitters act at specific receptor sites on the cell membrane. The threshold potential is the strength of electrical signal required to fire a given neuron. Excitatory neurotransmitters lower the threshold potential and make brain cells more sensitive to stimuli. Inhibitory neurotransmitters raise the threshold potential and make brain cells less sensitive. The threshold potential of a given cell is controlled by the balance between the NMDA receptor and the GABA receptor. The NMDA (N-methyl-D-aspartate) receptor is a receptor for glutamate, which is the most important excitatory neurotransmitter in the brain. Overstimulation of glutamate receptors causes slow, progressive death of nerve cells. GABA (gamma-aminobutyric acid) is an inhibitory neurotransmitter found in the brain. If you think of a spectrum of brain activity with seizure at one end and coma at the other, stimulation of the NMDA receptor shifts cells toward more alertness and better mental functioning, but if it is too active, it shifts brain cells too far, toward seizure and cell death. Stimulating the GABA receptor shifts brain cells toward the coma end of the spectrum.]
The point is that you need to block the NMDA receptor. We block it with magnesium; we use taurine to help magnesium, and we block it with a histamine blocker known as doxepin, since a histamine receptor sits right next to the NMDA receptor. And then we agonize the GABA receptor with Klonopin and Neurontin or GABA itself. Even valerian root agonizes the GABA receptor. [All of these chemicals act as substitutes for GABA to stimulate the GABA receptor and shift brain activity from seizure or cell death states toward coma and other healing states.]
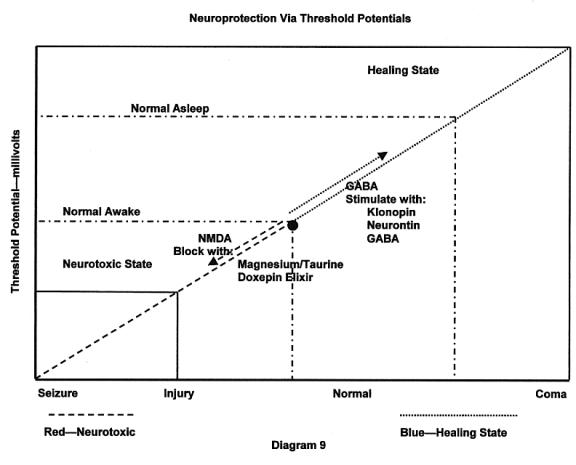
This diagram shows threshold potential on the Y axis from zero to infinity in millivolts. Normal awake is set here; normal sleep is set here, and so normal lies between these two dotted lines [Normal Awake and Normal Asleep], and in the daytime, you're here [Normal Awake], and in the night-time, you're here [Normal Asleep]. At this point right there [the round dot], at that threshold potential, your brain is optimized for function. You're best able to process information quickly and accurately, see essential information, screen out things that don't matter, and you feel like you're operating on all cylinders. Here is your sleep domain, although there are probably different levels of sleep; probably your threshold potentials vary slightly between Stage IV, Stage III, Stage II and Stage I sleep.
What sets this threshold is the opposing action of these receptors. On each membrane of each neuron in the brain, there are several of these two types of receptors or of similar receptors that do essentially the same thing as these two do. NMDA tends to lower the threshold potential when stimulated. GABA tends to raise the threshold potential when stimulated, and when they balance each other out, it sets the threshold potential at this optimum point [the round dot].
If you stimulate the NMDA receptor and drive the threshold potential all the way to zero, a zero threshold potential is a seizure, because the neuron is firing with no stimulus. If you go the other way and you stimulate GABA and drive the threshold all the way to infinity, then the neuron doesn't fire for any reason, and we call that coma, and normal is in between. What's interesting about this model is that the routine response of the brain to injury is to lower the threshold potential, so injury sits here. When the brain is at the injury point, it means that the neuron is firing at lower sensory thresholds. That means that you see everything and hear everything, that light is too bright, and noise is too loud, and people are too irritating, and shopping malls are too problematic, and making decisions is overwhelming, and you look for a quiet, deep hole to get into. You're having to modify your behavior because your brain cells are too sensitive; they're firing at lower threshold potentials. This has a dramatic effect on your functioning, and of course you don't sleep very well either, down here in the injury state.
But there's another thing that happens, that's called the neurotoxic state. At every point along the red line, all the way up to and including the normal awake state, the neuron is firing faster than it can detoxify the metabolic waste it's creating, from this rapid de-polarization [electrical activity]. So the toxins are increasing in the neuron, and how do you get rid of those toxins? At night, you enter the sleep cycle, which is the healing state, all along the blue line. At that point, the neuron is firing so slowly that you can re-direct energy reserves to the act of detoxification, because you don't have to use all your energy reserves to fire that neuron. The greatest healing state is the coma state. And there are actually whole books written on the healing properties of coma. I've often thought that what we should do is hire about six anesthesiologists, get six beds, and put all the CFIDS patients in coma for about a week or two, and when we bring them back, they're going to be a lot better. That has actually happened twice in my twelve years with this illness. Two patients ended up in comas unrelated to CFIDS and had dramatic clinical improvement after a week in coma, because coma is the ultimate healing state. Very deep sleep is also healing; deep sleep is healing; meditation is healing, but the normal optimal awake, alert state is actually slightly neurotoxic.
But CFIDS patients are sitting down here [in the injury state]. So what you have to do, in the daytime, you have to move them from the injury state to the normal awake state so that they think better and are less toxic, and at night, you have to move them into the healing state. And how do you do that? It's a simple matter of receptor manipulation. You block the NMDA receptor or you stimulate the GABA receptor, and best of all, you do both. Now isn't it interesting that magnesium is probably the very best NMDA receptor blocker, and guess who is deficient in magnesium? People with CFIDS. So the first and best drug for this whole thing, interestingly, is magnesium. It is also the drug of choice for seizures, because it pushes you instantly toward the healing state. CFIDS patients are already deficient, and that must be addressed. If you don't address that, then you're rowing upstream with anything else you do. It's a very powerful idea.
QUESTION: [Inaudible]
Injectable magnesium has always been clinically superior to oral magnesium. I think the reason is that if you take oral magnesium, it goes through the digestive system, enters the portal circulation, and goes through the liver first. The liver has, I think, a big need for magnesium, and probably takes a lot of it. So the result is an unequal distribution of magnesium in the body when what I really want is to get magnesium into the brain. If you inject magnesium, it's more equally distributed; every organ system gets its fair crack at the magnesium. So I've often found the shots simply work better. What I usually do is start off with the shots, plus some tablet supplements. The shot is given every day for a month; then it's given twice a week for a month, and then they go off, taking the tablets the whole time, and then I have the patient decide. If they say, "I felt much better taking it daily than twice a week," then they should take it daily. If they say "Twice a week was just as good as daily, but better than tablets," then they should take it twice a week. If they think, "I really can't tell any difference, shots or tablets," then they should take tablets. What I found is that about 70% of patients would choose the shots, and they'll usually choose them every single day, which is pretty amazing, given magnesium shots.
I used to give magnesium a certain way, until I decided to give it to myself once. Actually, my wife gave it to me. And after that experience, I said, "This hurts," and so I said, "We have got to figure out a better way." I began to manipulate the dose in conjunction with taurine, which is a very mild agent and temporizes [tempers?] the magnesium. We eventually got down to a dose of one-half cc. of magnesium sulfate 50%, which is about 250 mg. One-half cc. of magnesium sulfate 50% with one and a half cc. of taurine, and that gives you a 2 cc. volume, and the injection is given slowly and intermittently. So you'll inject half a cc. and hold, count to three or four, and repeat. And it's given in a deep hip injection; you can actually give it to yourself, because it's almost in the side of the hip. And if you give it at that concentration and do the slow intermittent injection, it actually doesn't hurt. Or if it hurts at all, it's just a mild ache that goes away. If you're pushing it too quickly, it hurts, so you just slow down. So it's a really nice way to give magnesium, and patients tolerate it really quite well. At the same time, we give magnesium glycinate. Glycine is the smallest amino acid; magnesium is chelated [bonded] to it, and the glycinate helps get the magnesium into the cells; you don't pee it out as easily, and we'll give maybe 100 to 200 mg. of magnesium glycinate in the morning, and 200 mg. at night, plus the shot, which is only 250 mg., at night. When we cut back the shots, we don't increase the tablets. If you ask the question, "Well, can you get toxic on magnesium?" at these levels that we're giving, if you had kidney disease, yes, you could. But if you have adequate renal function, your kidneys will more than handle that level of magnesium.
[Dr. Cheney highly recommends Klonopin as a GABA stimulator. He also believes it acts synergistically with doxepin to improve sleep--each increases the effect of the other. However, doxepin can cause morning drowsiness if the dose is too high--5 to 10 mg. or higher. One indication that CFIDS patients' brains are in an injury state is the effect of low doses of Klonopin. If you give low doses to healthy people, it makes them drowsy, because it moves their brains toward the coma state. But a low dose makes a CFIDS patient more alert, because it shifts brain cells from the injury state toward the point of optimum functioning. Dr. Cheney recommends low doses in the morning to help mental functioning. If the dose is too high, the patient becomes drowsy, but at the right dose, patients think better. After the patient finds the right morning dose, he or she can take the same amount at mid-afternoon and then three to four times the morning dose at bedtime to improve sleep. Dr. Cheney believes it may be appropriate to double the dose during severe relapses.
[Dr. Cheney uses Neurontin (gabapentin) in resistant cases to protect the brain, but thinks some doctors are using doses that are too high.
[On the other hand, Dr. Cheney points out that selective serotonin reuptake inhibitors (SSRIs), the class of anti-depressants including Prozac, Zoloft, and Paxil, work by increasing the firing of neurons. He believes these drugs can have bad effects when taken for depression for periods of several years, and they would be even worse for CFIDS patients.]
You'll notice, though, this doesn't treat any primary issue in CFIDS. All it does is buy time. It protects the brain from further injury by keeping it out of this red zone where the neurons either die or decouple from their dendritic attachments [the extended arms of the neuron]. The neurons are alive, but they're not connected to the network. It has been very pleasing for me to adapt this neuroscience research, which is more than ten years old, and even today, neuroscientists think this way. If you don't know what's wrong with the brain, but you know it's being injured, act to put it in the healing state. You move to put it in the healing state and keep it out of the injury state. Then you have the luxury of figuring out what's happening later. And we'll do the same thing here. It does have an immediate effect, though; if you move yourself from the injury state to the optimum point, you definitely think better. You may even be able to go to the grocery store and pick out food from the shelves, because you're not overwhelmed any more.
Treatment Step III, DNA Protection
Antioxidant Vitamins
Bioflavonoids
Extra Vitamin E
Special Supplements
Co-Q 10 (fat soluble)
Lipoic Acid (physiological dose)
Omega 3 & Omega 6 Essential Fatty Acids
Melatonin, (if needed)
Step III. DNA protection. This is an oxidant stress disorder [with damage being done by free radical toxins], so we engage in anti-oxidant protection. This is an area where Jeffrey Bland [??] has done a lot of work that I think is important in chronic illness in general. Chronic illness in general involves oxidative stress; certainly CFIDS is a chronic illness. Multivitamins, bioflavonoids, extra vitamin E, Co-Q 10, lipoic acid, although we keep this at moderate amounts because of the mercury issue. Essential fatty acids and melatonin if needed. Melatonin is a potent anti-oxidant.
[Dr. Cheney recommends multivitamins without iron or copper, because iron and copper can cause chemical reactions that can increase oxidant stress. He also recommends 2000 to 4000 mg. of vitamin C a day in addition to the amount in your multivitamin. However, he believes mega-doses of 10 to 20 gm. can be dangerous; they can actually increase glutathione deficiency. He recommends 400 to 800 I.U. of vitamin E a day.
[Co-enzyme Q 10 is a naturally-occurring anti-oxidant that is necessary for energy production and is essential in the protection of DNA. It can influence fatigue, muscle function, and possibly mental function. (A co-enzyme is a substance that acts with or activates an enzyme.) Dr. Cheney recommends at least 200 mg. of Co-Q 10 a day. It isn't easily absorbed in the digestive tract, so a sublingual form is best.
[Lipoic acid is a powerful anti-oxidant that increases the effectiveness of glutathione. Dr. Cheney thinks it might be the most important supplement in this group, for protection of the central nervous system. He recommends 100 to 300 mg. a day. Lipoic acid can bind with mercury and allow it to be excreted from the body; however, it can also mobilize mercury--simply remove it from where it has been stored and redistribute it to other places in the body. Therefore, higher doses should be avoided.
[Essential fatty acid supplements include omega-3 oils, found in fish oil and flax seed oil; and omega-6 oils, found in borage seed oil. A balanced source includes both kinds.
[Melatonin is a brain chemical involved in regulating sleep patterns; it is sometimes used to reduce the effects of jet lag.]
One that needs to be emphasized is bioflavonoids. Antioxidant vitamins [vitamin C and vitamin E] can actually increase oxidative stress and can make you worse, unless you couple them with plant bioflavonoids. It's very important to add that to the mix. [The plant bioflavonoids include proanthocyanadins, quercetin, sylmarin, green tea, and ginkgo biloba. Proanthocyanadins include pycnogenol and grape seed extract, which are powerful anti-oxidants that act primarily in the brain. Quercetin is a bioflavonoid with antihistamine and anti-inflammatory properties. It should be taken with vitamin C. Sylmarin, or milk thistle extract, is an anti-oxidant that acts primarily in the liver. Green tea appears to have many positive health effects; however, it contains caffeine. Research has suggested that ginkgo biloba can improve mental functioning. Even if the patient doesn't notice a decrease in symptoms, anti-oxidants and other neural protection treatments can be providing benefits by protecting the nervous system from further damage.]
Treatment--Step IV, Neuroprotection from CNS Toxicity
CNS [central nervous system] Xenobiotic Detoxification
Parenteral [injected] Hydroxycobalamin (Vitamin B-12), starting at 10,000 mcg IM [intramuscular injection] HS [at bedtime]
CNS Homocysteine Detoxification
Pyridoxal-5-Phosphate
Folic Acid
Trimethylglycine
L-Serine
Protection for the brain. B-12 protection is paramount here. B-12 may act as a neuroprotective agent because it binds to nitrogen waste toxins in the brain, and the brains of CFIDS patients are known to be deficient in B-12. We use very high doses of hydroxycobalamin. The ordinary version of B-12 available in pharmacies is cyanocobalamin. It should never be used. It is not good as a detoxifying agent because it's cyanide hooked to cobalamin. If it decouples, you just trade one toxin for another. Hydroxycobalamin is water and cobalamin, and when it decouples you get free cobalamin; it binds to nitrogen residues and eliminates a fat-soluble toxin from the brain. But you need very high doses to do that. I've chosen this particular dose because studies in New York by Newbold [??] have shown that this high a dose, given over a decade, has been safe and effectively used against chronic illness.
We also protect against homocysteine, using a homocysteine-protective grouping. [Pyridoxal-5-phosphate is an activated enzyme form of vitamin B-6. Folic acid is another of the B vitamins. Trimethylgycine is a methyl donor; it provides a methyl group, a substance required for many important biochemical processes. It is believed to be effective against homocysteine. L-serine is an amino acid involved in important metabolic processes.]
Treatment--Step V, Toxic Source Attenuation
GI Tract Microbial Toxicity Source
Olive Leaf Extract
S. Boulardii (for limited time)
Organic Botanical Extracts (for limited time)
Glutamine Source
Polymicrobial Probiotic without FOS
Oral Cavity--Microbial Toxicity Source
Herbal Tooth and Gum Tonic
Remove or detoxify RCT [root canal teeth] and Cavitations
How do we get toxic source attenuation? To reduce the microbial toxic source, we use olive leaf extract. It has potent broad-spectrum antimicrobial effects, and can even be used to suppress gut bacterial overgrowth. S. Boulardii is a type of yeast that doesn't stay in the gut, but acidifies the gut, which promotes the friendly bacteria and inhibits unfriendly bacteria. We tend to only treat for a short time with it. Organic botanical extracts; we use pau d'arco, uvi ursi and wormwood and black walnut in liquid extracts, and we only treat for about a month at a time. These botanicals have been used for thousands of years by indigenous peoples to protect their guts from parasites, yeast, fungus, and bad bacteria, and so we figured they might be useful to push things more toward a normal gut ecology. [Dr. Cheney recommends 15 drops each of pau d'arco extract, uvi ursi extract, and wormwood/black walnut extract, one month on and one month off.] Glutamine source, very good for cell function in the gut. [Glutamine is the most abundant amino acid in the body. It is necessary for immune system functioning, and it is important in maintaining the health of the lining of the intestine and preventing harmful intestinal bacteria. Glutamine is available in various supplement forms.]
Then a polymicrobial probiotic without fructo-oligo-saccharides. You don't want to use a probiotic with FOS, because FOS is simply fertilizer for the bad bacteria and makes them grow faster. [Probiotics are sources of healthful microflora. A good product will include acidophilus, bifidum, rhamnoses, and possibly others. Dr. Cheney recommends a product called Flora Source, which has 15 billion units and 14 bacteria strains per capsule. It is available from NEEDS, 1-800-634-1380, www.needs.com]
What do you do to reduce mouth microbial toxicity? The simple and quick thing to do is an herbal mouth rinse that keeps your mouth squeaky-clean, and then in certain individuals, we may investigate root canal teeth and cavitations for possible removal or detoxification, and that's about an hour long talk, just to go through the ins and outs of that. [I haven't been able to find any information on what the herbal mouth rinse is.]
Treatment--Step V, Toxic Source Attenuation
Heavy Metals (Load & Toxic Potential)
Amalgams--Be Very Careful About Removing
Fish
Water Supply
Home Environment
Home Mold Plate Testing
Air Duct Inspections & Cleaning
Electronic Air Duct Inserts--Mold
HEPA/HEGA Air Filters [high-efficiency particle adsorption, high-efficiency gas adsorption]
Personal VOC [volatile organic compound] Badges (3M)
Carbon Monoxide Detectors
Heavy metals could be very important in certain individuals. [Heavy metals are a group of toxic metallic substances like lead, arsenic, cadmium, and mercury.] Amalgams [silver-mercury amalgam tooth fillings] are the biggest sources; they also come from fish and water supply. [Because of water pollution, fish from many rivers contain dangerous levels of mercury, and mercury and other heavy metals are present in many city water supplies.] The important thing about heavy metals is to realize you can do load testing and toxicity testing, and they are not the same. [Load testing measures the total amount of the toxic substance.] There are people with high loads that are not toxic; there are people with low loads that are very toxic. So you have to differentiate between load and relative toxicity, and that can be done. That's a very important first step. And then the next thing to do, if you plan on removal [of tooth fillings], is to be very, very careful. Removing mercury can move you from the frying pan into the fire. You can go from feeling bad to feeling very bad. Mercury extraction can be very convoluted and complicated, and a difficult choice for some patients, and that's about another hour discussion.
Home environment. I like the home mold plate testing. You order these from Sherry Rodgers' lab in Syracuse, N.Y. You get three mold plates; you open one up in the bedroom, one in another room that you spend time in, and one in the worst room in the house. You open them for an hour at waist height, close them back up, send them back to Syracuse, and they'll give you a printout of all the types of mold growing in your house and give you the colony count. [Dr. Sherry Rodgers is a physician and an expert in environmental medicine. The plates can be ordered from Prestige Publishing, the company that publishes Dr. Rodgers' books, 1-800-846-6687. Dr. Cheney says the plates cost about $10 each; the Dallas-Fort Worth Support Group website says they are $27.50 each, so if you're interested, you'll have to call Prestige Publishing and ask. After you return the plates, you will receive the results in 10 to 12 weeks.] That gives you a nice overview of whether you have a mold problem and how serious it is. You can then do IGE-specific blood testing [which tests for allergic reactions to the specific types of mold], and that tells you if you're even being bothered by that mold. You may or may not be. Air duct inspections and cleaning may be important in mold removal, engineering inspections of the home as well. Electronic air duct inserts are very good for getting rid of the mold and very inexpensive. HEPA/HEGA air filters are good for all kinds of indoor air quality issues.
The 3M Company makes a personal volatile organic compound badge. I think you wear it for two days, and send it to 3M, and then they can actually measure the amount of all volatile organic compounds you've been exposed to, or the amount of specific ones like formaldehyde, or benzene, or some other organic compound you're specifically concerned about. Very interesting device. [Volatile organic compounds are chemicals that evaporate quickly and produce toxic gases. VOCs include gasoline, lighter fluids, and other fuels; other automotive products; paints, paint strippers, and solvents; some aerosol sprays, cleansers, and disinfectants; many glues and other hobby supplies; moth repellents and air fresheners; and dry-cleaned clothing. For more information on VOCs, go to the U.S. EPA website: http://www.epa.gov/iaq/voc.html] And then carbon monoxide detectors. I've had some terrible situations with CFIDS patients who I know had CFIDS, but they had carbon monoxide poisoning at the same time, and you always need to think about that, especially if you have gas or oil heating.
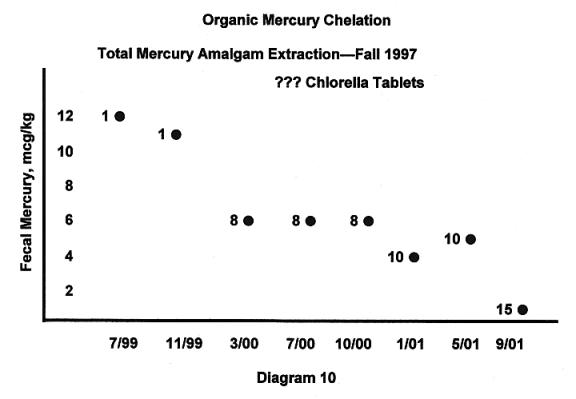
[Chelation is a method of removing heavy metals from the body by administering substances that chelate or bind to the metal; the heavy metal is then excreted along with the chelating agent.]
I wanted to show you this particular slide on mercury detoxification, because I think it's so interesting. This is a patient who had her amalgams removed in the fall of 1997. This is her fecal mercury level. By the way, mercury in the stool is the most accurate measure of load. Hair mercury, blood mercury is not a very accurate measure of load. Post chelation challenge may also not be particularly accurate of load. [A post-chelation challenge test consists of administering a chelating agent such as DMSA (discussed below) to see if more mercury can be removed.] But stool mercury is pretty good base line for mercury. And she had pretty high fecal mercury. And she started on one tablet per day of Chlorella, which is a green algae, and she could not tolerate two. Two green algae made her really, really sick, and if two green algae tablets make you sick, it's very suggestive of mercury toxicity. But after about six months, we were able to get her to eight tablets, and it dropped her mercury to here. Then we got her to ten tablets, and she dropped to here. She was using ten tablets, and then she had this kind of rise, which is typical. Sometimes when you go up to these higher levels of chlorella, there's initially an increase in mercury excretion, followed by a decrease. And then we put her on fifteen tablets, and she got all the way down here, and by the way, this particular number, which is .009 mcg./kg. is essentially zero. You basically can't get any more mercury out of her with this particular heavyduty chelator, although I don't think it's as heavy-duty as some of the pharmacologic agents out there. And the point is, you can use simply green algae. It takes two years to do this, but it's a way to remove mercury far more safely than the use of what I call the pharmaceutical approach, with DMSA, DMPS, which, although more efficient, run the risk of mobilizing far more mercury and causing potentially more trouble. So I kind of like the chlorella, and it really does work. [DMSA is dimercaptosuccinic acid. DMPS is sodium dimercaptopropanesulfonate. Both are used as chelating agents for removal of mercury from the body, although there is disagreement over their effectiveness and the risks involved.]
Treatment--Step VI, Detoxification; Beware of Toxic Mobilization
Hydroxycobalamin (start at 10,000 mcg. per day)
Methylsulfonylmethane (MSM at 6 to 12 g. per day)
Whey Protein Concentrate (10 to 20 g. per day)
Guaifenesin (short acting, start at 300 mg. every 12 hours)
Growth Hormone (0.2 mg SQ [subcutaneous injection] MiniQuick Q week [once a week])
[Genotropin MiniQuick is a brand of growth hormone supplied in pre-filled syringes.]
Detoxification. Beware of toxic mobilization. Hydroxycobalamin, MSM, whey protein, guaifenesin, and growth hormone. I've already talked about that.
Treatment--Step VI, Novel Forms of Detoxification
Colon Hydrotherapy (Should Be Time Limited)
Hydrogen Peroxide/Epsom Salts Bathing (BIW [Twice a Week])
Infra-red Light Pads Over Lymphatic Drainage Sites 20 to 40 minutes TIW [Three Times a Week] (Activates NOS3)
Deep Tissue Massage (BIW [Twice a Week])
Infra-red Sauna at Low Temperature TIW [Three Times a Week]
Novel forms of detoxification. Some of these we're beginning to explore in CFIDS patients, and I think some of them will pan out. Colon hydrotherapy [enemas] should be time-limited, but could be a way to help certain people with really bad guts, really bad colons. Hydrogen peroxide bathing with Epsom salts twice a week could be very interesting. Infra-red light pads over lymphatic drainage sites. It basically activates the nitric oxide synthetase3 enzyme and may have some other properties that may dramatically increase detoxification. [I believe Dr. Cheney is referring to endothelium nitric oxide synthase (NOS3), which I think is involved in production of nitric oxide. Nitric oxide is involved in many physiological reactions, and white blood cells produce large quantities of nitric oxide to kill bacteria and parasites.] Deep tissue massage and infra-red sauna at low temperatures. All of these we're in the process of exploring, and we feel that detoxification, although important, is a two-edged sword in this disease. If you go too fast, you get sick, so you have to keep on the safe side of tolerance for CFIDS patients.
Treatment--Step VII, Enhancing the Phase III Recovery Trajectory
Growth Hormone Injection (Once or Twice a Week)
Fetal Bovine Growth Factors (Twice a Week for a Limited Time)
Mesenchyme
Liver, Thymus, Adrenal, Brain
Enhancing the Phase III recovery trajectory. Growth hormone and fetal bovine growth factors are probably the best way to do that. [Mesenchyme is a type of undifferentiated tissue of the early embryo. Individual mesenchyme cells migrate to different parts of the body where they form most of the skeletal and connective tissue, the blood and the blood system, and the smooth muscles of the intestines. The thymus gland in the top of the chest is the source of the immune system's T-cells, which are named for it.]
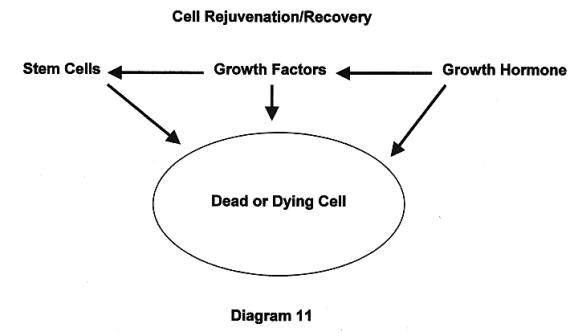
Here's a cell that's either dead or dying. It's rejuvenated by growth hormone, by growth factors, or by stem cells, and each of them can have an effect on this dying or dead cell. Growth hormone is the most important one in some ways, because it controls growth factor expression, which in turn controls stem cell migration, differentiation, and integration into the network. Of all these three things with rejuvenating effects, the one thing we know is affected in CFIDS is growth hormone. The point is that if you don't address this, it may be impossible to address the dead cell or the dying cell and achieve cell recovery and rejuvenation.
[Dr. Cheney believes that Greta Moorkens' work proved that CFIDS involves growth hormone deficiency. (Moorkens, Greta, "Endocrine and Metabolic Aspects of the Chronic Fatigue Syndrome," Ph.D. thesis, May, 2000, Antwerp University, Belgium)
[Growth hormone is produced by the pituitary gland; it stimulates the growth of muscles and bones and helps regulate metabolism. Growth hormone helps maintain blood sugar levels for the brain and stimulates the breakdown of fat into sugar so it can be used to produce energy. In many cases, growth hormone appears to work by activating a number of growth factors.
[Growth hormone is also associated with stage IV sleep. Without growth hormone, you don't get enough stage IV sleep--but lack of stage IV sleep reduces growth hormone production, creating a vicious circle.
[Exercise should cause a big spike in growth hormone. Exercise breaks down muscles, and a normal body responds by increasing growth hormone to build up the muscles. In fact, it builds them up stronger than they were before; that's the effect of training. But if you don't have enough growth hormone to repair the muscles, and if you continue to exercise, the muscles get weaker.
[Lack of growth hormone can cause other hormones to become ineffective, even though they are at normal levels. That's because growth hormone is necessary for the functioning of the receptor sites where other hormones take effect.
[Without sufficient growth hormone the body can't synthesize proteins, which are essential for normal cell function. So CFIDS begins with protein synthesis disruption caused by RNase-L, and it ends with protein synthesis disruption caused by growth hormone deficiency. This continued disruption of protein synthesis explains why so many patients don't make progress even though they're doing all the right things in terms of supplements, detoxification, and other measures.
[For a long time, it was believed that adults had no stem cells in their bodies, but Dr. Cheney cites research showing stem cells in the brain of a 60-year-old man. He believes it isn't necessary to put stem cells into the body to produce healing; it's only necessary to activate the stem cells already there. He believes human growth factors aren't necessary for healing; it can be done with growth factors from other mammals. He cites research showing that injuries to monkey brains can be repaired with bovine growth factors (from cattle). The growth factors will stimulate stem cells to differentiate into whatever kind of tissue is needed for healing. Then growth hormone will stimulate sufficient protein synthesis to complete the healing.]
Growth Hormone/Growth Factor Study. Preliminary Results
Nine have completed or are poised to complete the study
6 of 9 or 67% are responders (good to excellent)
Three are either on hold or are very early in the study--too early to tell
We have preliminary results of our study on growth hormone and growth factor. Nine people have completed or are poised to complete the study. Six of nine, or 67%, are responders, and I rate them from good to excellent. Three are either on hold or are very early in the study, and it's too early to tell. Just two days ago, I processed data on two who have completed the study, and it's really an amazing story of this mother and son. The mother is a chamber musician who could not play and is now on the road with her daughter playing chamber music again after this treatment. Her son, who washed out of Brown University because of CFIDS, is now full-time at Brown again. Another patient said that before the treatment, "I sat in front of the television set all day long and that's all I did," and now she has opened up a business again. Another patient who was a dance instructor is now a full-time dance instructor again. So clearly we have seen some really remarkable, excellent responses on this regime.
But there have also been some negatives. We've had three nonresponders, and all three of them were male, and all of them developed joint pain, fairly significant joint pain, particularly in the wrists, and two of them actually required steroids to treat it. This is mentioned in the literature as a side effect of growth hormone, although they didn't get it from growth hormone; they got it from growth factors. I should also add that I split the group into an immune-modulated and treated group and a non-immune-modulated and treated group, and these men were all in the non-immune-modulated group. So I think it's very important to immune-modulate first, so that you're not giving growth hormone or growth factor to an immune up-regulated state, which would only turn on that system even more.
Growth Hormone/Growth Factor Study. Preliminary Results
Growth hormone must be kept at low doses given once or twice weekly
Patients must be immune modulated before starting GH or GFs
Growth factor dose needs to be adjusted downward similar to GH
Growth hormone must be kept at a low dose given once or twice a week. If you push it too high, you can reinforce some of the pathophysiology of CFIDS. You can reinforce the viral re-activation events, because viruses will grow faster under the influence of growth hormone. You can reinforce the immune activation state and activate it even more. In order to prevent that, patients must be immune modulated before starting growth hormone, and the growth hormone dose must be kept low. And the growth factor dose, I think, needs to be adjusted downward, similar to growth hormone, and we largely were unable to do that because of the way it is packaged.
QUESTION: Review again the risks and downside of taking growth hormone and growth factors, and distinguish between the risks.
In some ways, the risks and the benefits are very similar. Think of growth hormone as a broad-spectrum controller of protein synthesis throughout the body and in all cells. Growth factor is more specific in increasing protein synthesis of specific cells or specific DNA sites for specific effects. So it's a little more narrow in scope. Growth hormone has a very broad scope. But except for that, I think they should be viewed as somewhat similar in terms of the risks and benefits.
The risks of growth hormone: the one talked about the most is the cancer risk. If you have an active cancer or you have been diagnosed with cancer within five years, and you're trying to find out if the cancer has been cured, you should not take growth hormone. Growth hormone in test tubes has been known to increase cancer growth rates because it increases protein synthesis rates. In animal models, however, it's not quite so clear, because giving growth hormone to some animals with tumors will actually shrink their tumors. In others, the tumors grow. Growth hormone can improve immune function, which will fight the cancer; if that happens, then you win. If cancer growth increases more than immune function, then you lose. The problem is that we can never tell which way it might go, so the conservative approach is not to give growth hormone to a cancer patient. It should be said that growth hormone does not cause cancer but rather can make cancer grow faster. I think it should also be said that the growth hormone dose we recommend is minuscule; it's almost a pediatric dose given once a week, so we're not giving physiologic levels of growth hormone. So we think the cancer risk is far below what you would get with a physiologic dose.
The other risks I think are more real and more of a concern for CFIDS patients, and one risk is that you could activate a virus. So if you were having 600,000 HHV-6 strain A viruses growing per cc. of blood, and you're injecting yourself with growth hormone, you could ramp that up to 800,000, because growth hormone will make viruses grow faster just as it makes cancer grow faster. I have seen patients on growth hormone particularly when we go to higher doses initiate what seemed to be a viral syndrome, and it continued even when I brought the growth hormone back down. Once you set it off, it can remain active for some time.
Another problem is that some patients have experienced what I call a toxic reaction to growth hormone, which may be RNase-L-induced. RNase-L is a protein; growth hormone can increase production of that protein. RNase-L, if activated, could impair liver function, giving you more toxicity from your portal circulation. So these are real issues that CFIDS patients face when they take growth hormone, and what we've found is that what's important is to keep the growth hormone at a very low level. The level that we keep it at, where we do not seem to see trouble in 99.9% of cases, is .2 mg. once a week. At that level, we just haven't seen any of those problems. But as soon as we go up to .4 mg. once or twice a week, or .6 mg. once or twice a week, some of these patients begin to have problems. Probably one in three will have problems at .4 mg. and maybe more at .6 mg. So we made the decision that those doses were too high, and we would operate at a level where no one got a problem and hope that .2 mg. a week would bring long-term benefits. And my sense is that in most cases it does, but the benefits come more slowly. It's more like month by month, year by year, you just get a little better. Nothing dramatic, but just a sense that you're getting a little better is what we generally see at .2 mg. a week. We could go faster, but if we do, some patients may run into trouble. We do have some patients who are not so risk-averse, and they're willing to accept some risk here and may go to .4 mg.after a while and go a little faster.
Another thing I've noticed is the better the patients' condition is when they start on growth hormone, the better they do. Growth hormone is particularly advantageous in the patient who has been through the worst of it, has come up onto a plateau of functioning, and is maybe 20% to 30% away from where they used to be. That is the ideal patient to treat with growth hormone, the one who will get the most benefit and is least likely to have problems. If you give it to the extremely sick individual, I think that's the person that sometimes seems to get the least benefit, and can be the most likely to have a problem, though not at .2 mg. once a week.
Growth factor is pretty much the same. If there's a difference, it is that growth factor seems to have a greater propensity than growth hormone to activate the immune system, and we think it turns on tumor necrosis factor-alpha, because of the joint pain that we see. TNF-alpha [a cytokine that triggers destruction of tumor cells] is famous for causing joint pain, which is why the newest and best rheumatoid arthritic drug is a TNF-alpha blocker. Growth factor seems to turn on that cytokine.
When you add growth factors to growth hormone, the functional response seems to be much better than either growth hormone or growth factors alone. The problem with growth factors is that it comes in an 8 cc. bottle that's frozen, and once you thaw it, you have to use the whole thing, and I think that for a lot of people, that might be ten times more growth factors than they need. So you'd be taking a tenth of that and wasting nine-tenths of it, and that's a huge waste of money. So unless the company repackages it in very tiny vials, I think it's not going to be a very practical treatment for a great majority of patients. But the study results are promising. I first thought, no, we're never going to do this again, but the quality of the response has been so good that I'm having to re-think that. I may re-think it again after we analyze all the data that we acquired in this one-year study.
QUESTION: How and where can I be treated with Ampligen?
You can get Ampligen on either the 516 double-blind placebo-controlled trial or the 511 open-label trial, in which you pay for it. The problem is that the company has filled the 511 easily and has trouble filling the double-blind placebo-controlled trial, and apparently has cut off the 511 unless you are disqualified from entering the 516. So unless you have a disqualifying condition for 516, you can't even get into 511 these days. That means that most people can get Ampligen only by entering 516, which means a 50% chance you'll get saline [the placebo] for six months, and then Ampligen for six months. The other problem with Ampligen is that the summer of 2003 is supposed to be the end of Ampligen testing, which means that either the company will apply for and get approval from the FDA to market this drug for CFIDS in this country, or they're going to shut down operations. So we're now a year and a half away from either having it available and paid for by insurance or not having it available at all. So if there's only year and a half window left, and of course if you're in 516, half the time you're on saline, I think that the opportunities for Ampligen are not particularly bright right now. Then it can cost $30,000 a year to receive Ampligen, and probably only about 50% of people truly respond to it.
QUESTION: Should CFIDS patients with high cholesterol be treated with anti-cholesterol drugs? Should we avoid using the higher-grade anti-cholesterol drugs, the statin drugs, the drugs that inhibit cholesterol synthesis in the liver? How much are we truly at risk for heart disease?
My thinking on this is that very few people with this disease should be given cholesterol-lowering drugs, especially the kind that inhibit cholesterol synthesis in the liver. And the reason for that is that the drug that lowers cholesterol also lowers co-enzyme Q 10. In fact, even in the PDR [Physician's Desk Reference, which lists information on all prescription drugs], it says lowers Co-Q 10 a full 40%, and CFIDS patients have been shown to have at least a 50% lowering of Co-Q 10, already. Then the drugs would reduce it another 40%. So that may explain why, when physicians have given anti-cholesterol drugs, a lot of these patients crash and burn, just get really sick on anti-cholesterol drugs.
Secondly, I suspect that there's another reason you ought to worry. What does the body do with cholesterol? It makes steroid hormones from cholesterol. It makes testosterone, cortisol, aldosterone, estrogen, progesterone, and DHEA from cholesterol. Production of these steroid hormones are affected in this disease, so we know our patients have low levels of all of them, and what would the body do, staring at all this low steroid synthesis? It would say, "I think I need more cholesterol to make more of what I'm low in." So there's probably some feedback going to the liver to say, "Make more cholesterol, so I can make more of these steroid hormones." So you can guess what's going to happen when you take a drug that ignores that feedback and savages the synthesis of cholesterol in the liver; your cortisol levels drop sharply, and you really get sick. So I think what really clobbers CFIDS patients is that they start out adrenally insufficient, and those cholesterol-lowering drugs make them really adrenally insufficient, because they can no longer synthesize those steroid hormones any more since they're synthesized directly from cholesterol. So I can't think of a very good reason to treat with a cholesterol-lowering drug.
What's the risk of getting heart disease if you have CFIDS? Heart attacks and coronary artery disease in CFIDS are very, very rare; it's just something I don't see. The average age of my patients used to be 38, but I'd say it's probably 48 by now. So at 48, you should be seeing some coronary disease, and I have a lot of 58-year-olds, and I just don't see it. They have low blood pressures, really low blood pressures, which reduces coronary risk. So I don't think it's something they're at great risk for, although familial issues might be important here. So I think every case is an individual case, and there may be some-one with CFIDS, and everybody in their family has died of coronary disease by the age of 45 and they're walking around with a cholesterol of 400, and yes, maybe they need a cholesterol-lowering drug. So I can't speak to that isolated individual, but the average case of CFIDS with a cholesterol of 240 should not be treated with a cholesterol-lowering drug.
QUESTION: Could you tell us what it would be like to go through your CFIDS program? What tests would you usually order, and how long would initial testing take?
Going through our program is sort of like this lecture: it's long and complicated. But some people walk out of our clinic and say "I now know more than ever I wanted to know, and I never want to know anything like this ever again." So if you're the kind of person that says, "I don't want to know what's wrong with me; just treat me and get me well," I'm not a very good person to see. If, on the other hand, you're one of these people who say, "I really want to know what's going on, and I want to take control of this myself, and I don't want to leave this to anybody. I know I take care of myself the best, and I want to participate in my care; to do that I have to be an informed person, and I want to know everything there is to know."--then our clinic is a good place for you to come to. So when you come to our clinic, the first day we spend a lot of time getting clinical information; we spend about half a day on a history. And then on the second day we end up talking about treatment, much as we've been doing today, and sprinkled through the whole thing are discussions on pathophysiology, which is really an attempt to transfer power from me to you so that you know as much as I do about this disease, and maybe you can make your own decisions about what you would like to do or not like to do, based upon the data that is given you.
A lot of the tests we order are really tests to prove that you have some of this pathophysiology. Do you have elevated RNase-L? Do you have elevated EBV, CMV, HHV-6, HHV-7, Mycoplasma, Chlamydia pneumoniae titers by Taqman assays? Do you have a coagulopathy? Do you have excess soluble fibrin monomer? Do you have TH2 activation and TH1 suppression? Do you show toxins in your urine that correlate with gut-derived xenobiotic toxins? Is your stool loaded with mercury? How do you respond to chlorella in advancing doses, which is a measure of heavy metal toxicity. We measure growth hormone. We measure it by two methods now. We measure exercise growth hormone increase. If you're normal, it should rise at least to ten nanograms, and most of our patients don't even get above one nanogram. We even do ITT tests, insulin tolerance tests. [An insulin tolerance test involves injecting insulin and measuring the effects; it is used to measure growth hormone, cortisol, and ACTH, adrenocorticotropic hormone, which stimulates the production of cortisol.] We do arginine challenge tests [to measure growth hormone], and recently we now have a 24-hour urine test for growth hormone, and I think that and the exercise test are probably going to be our best tests for growth hormone. We measure cortisol response to exercise. So basically we do enough testing to make sure that you fit the model of this disease.
How long do the initial tests take? We basically have gotten out of the testing business. We don't really test anyone, except for a couple of things that we really have to test because it's the only way to do it. But for all the other testing, we fax the order to the labs and the labs send you the kit. It has the tubes in it and the drawing instructions, and you ship it back to the lab, and you contract directly with the lab, so you get the lowest possible price. Most people will get nine or ten kits coming to them in the mail. Now I've had some say, "That's a lot of work," to get all these nine kits done, and it is a lot of work, but we could bring all that work into my clinic and then charge for that, and then the price for the tests would be significantly greater. We chose the way that's cheaper for the patients.
QUESTION: What do I think of oral thymus?
Well, thymus is a glandular product, and we have used glandulars in this disease, particularly adrenal glandulars, with some success, and a thymus glandular makes sense to me. The only problem with glandulars is that they're derived from animal products, and if you're using animal products, then you have to worry about mad cow disease and other risks of animal-derived products. So we sort of moved a little bit away from the glandulars, although I certainly have no problem conceptually with a glandular.
QUESTION: What impact does Martin's stealth virus have?
Martin's stealth virus is just another virus out there that could be involved in initiating CFIDS. I doubt it's the only one, but it certainly could be one. [W. John Martin, M.D., Ph.D., has developed a theory of stealth viruses that the immune system does not detect, because they do not have antigens on their surfaces. Such a virus would not trigger a response by the immune system to fight it. For more information on Dr. Martin's theories about stealth viruses, see http://www.ccid.org/about.htm#]
QUESTION: Does CFIDS affect early aging or premature natural death?
Very interesting question. Some CFIDS patients look remarkably younger than stated age, and some look remarkably older. And If I had to say what the difference is, if you have this disease, and you accommodate to it, and stay within boundaries, I think you can actually significantly forestall some of the age-related phenomena. But if you don't do that, and you push ahead--I'm reminded of one patient; she will not stay within her boundaries; she consistently pushes beyond her boundaries, and she looks a hundred years old, and she's about 40. She looks terrible. So you have to gauge your body and not over-extend it with this illness.
QUESTION: Do you have any ideas regarding EEG [electroencephalogram] biofeedback as a treatment for FM/CFS?
We've engaged in EEG biofeedback, and I think it can work in a limited fashion. The problem is that the improvement doesn't last. You'll see a benefit, but it doesn't seem to last. That's been my experience with EEG biofeedback.
Thank you very much.
© Campaign for an Irish ME clinic. Charity number APP 21042.